download the Powerpoint here: electrolysis presentation for trans ohio symposium
somone uploaded it here as well but have asked it to be removed as i didnt, ya know, lol
otherwise take it as a compliment someone thought it important enough… that somone is the emancipated electrologist- whose working with others to erase me because non of them want trans people to have face and genital hair removal under medicaid cause itll devalue their feilds hourly rate.
https://fr.slideserve.com/morison/medical-necessity-of-electrolysis-powerpoint-ppt-presentation
heres anouther attempt to move it away from my site, this is what hostile takeovers look like in business. do all this work an then someone wants to steal it an claim it for themselves, whatever, do it then, start performing hair removal under medicaid for poor people whod never afford it..
https://slidetodoc.com/medical-necessity-of-electrolysis-in-transgender-patients-kittysbelle/
theyll prolly try to write a book instead of the eventual medical paper that is this work, to some degree this blog page could be considered the “Unoffical Mike Bono” as he has been the most help out of everyone who has ever contributed to those archives. the reader should understand i pulled something from the community files he wrote on hair tell from 30 yrs ago and applied them to modern context with the affordable care act extensions in 2016. understand im using it to benefit the entire community, the poor not served simply from consequance of business interests. i thank you for building HairTell its great resource and i highly recomend it to everyone. ive seen information go missing since our existence went against AOL ToU, which is why i stored it here intially. would hope to be considered an addition not a detraction by anyone this work helps one day.
This work is dedicated in memory of Donna J Noble, CTE, liscenced cosmetic therapist in Ohio between 1990 and ___. She was my first and favorite electrologist and can be accredited with clearing the bulk of my upper-lip while wrangling my eyebrows to a state of normalicy.
https://www.manta.com/c/mmndc4n/donna-j-noble-electrolysis
https://citylifestyle.com/cincinnati-oh/businesses/beauty/noble-donna-j-ct-549086
Her husband had built a nice addition to the back of their house solely for her to work in due to warren county codes requiring separate air flow from a kitchen. The monetary discount she afforded me out of sympathy i presume, though there’s a connection to my grandma through their church, was my first introduction to finances and forced me to prioritize. Sadly I still owe her for the last touchup treatment when i was homeless, right befor i tried a new city. Work she did probably saved my life; a terminal upper lip is visable even clean shaven, it allowed me to pass in day to day interactions affording some degree of diversion from the violence that consumes too many of our lived experiences.
I’m attempting to pay it forward.
The following is my research from a patient perspective, along with further elaborations, using the powerpoint as a sort of section guide to works cited :
*updated for Nov20th, 2020
Not only can most not fathom being born “wrong” but the repercussions of not being able to interact with others in the most social sense, if not the basest. Gender Incongruences, encompassing what was formerly known as Gender Dysphoria, are experienced to different degrees by those of biologic variance. The relation too oneself in a cishetronormative world- not only forces the afflicted to overcome harsh social constructs equivalent to banishment from peers in our current society, for some of us it effects our ability to function, reproduce, or to ever develop physical relations in “knowing” another human being on a relationship level.
Yet what i want to get through to you in this is something as common and unforgiving as HAIR.

If you accept the fact that brains are mosaicly sexed organs to infinite degrees, including instances of crossex adaptability, then one must include the complete nervous system as lending itself to what that brain perceives. in the epidermal, nerve endings are in bundles, around the root of each and every hair. A primitive form of extrasensory perception to most, unrelenting waves of dirty stitches sending signals of alienable wrong to others. A sexed brain would have evolved to expect certain structures based upon the sex hormones typically introduced directing expected growth at certain periods of a bodies development. the mental map of what the body should be is constantly under attack, what is termed “dysphoria” is in reality an utter revulsion from a form that seems to be attacking itself. “This isn’t me, this is not self”. The central nervous unit is receiving signals from the genitalia and elsewhere, that somethings “wrong”, these should not be exposed and vulnerable but safely tucked inside.
“The human genital tubercle differentiates into a penis under the influence of androgens forming a tubular urethra that develops by canalization of the urethral plate to form a wide diamond-shaped urethral groove (opening zipper) whose edges (urethral folds) fuse in the midline (closing zipper). In contrast, in females, without the influence of androgens, the vestibular plate (homologue of the urethral plate) undergoes canalization to form a wide vestibular groove whose edges (vestibular folds) remain unfused, ultimately forming the labia minora defining the vaginal vestibule. The neurovascular anatomy is similar in both the developing human penis and clitoris and is the key to successful surgical reconstructions. The male scrotum and female labia majora come from the same embryonic structure called the labiascrotal fold. The paired dorsal erectile tissues called the corpora cavernosa are found in both the penis and clitoris. The head of the penis and clitoris both come from the embryonic genital tubercle.” Ken Saladin, Emeritus professor of biology and author.
https://urology.ucsf.edu/sites/urology.ucsf.edu/files/uploaded-files/attachments/4_s_development_of_the_penis_and_clitoris_1-s2.0-s0301468118300938-main.pdf
Now imagine those dirty stitches growing out of a woman’s face, or out of her vagina that threw itself up thru virilization. The psychological/physiological torment of plucking-burning-razing only to have it return in ever thickening waves, The deformity be-twix our legs that caused all of this, also requiring permanent removal of hair in preoperative steps, before surgical correction of the area can happen. Too the the afflicted this is not merely some life affirming aesthetic body work, this is a cruel constant untreated aggravation. Something that happened beyond our control, something that at one time was preventable through puberty suppressants now practiced on the youth, something that has a cure; held out of reach by discrimination, bias and ignorance. Laser and electrolysis are both seen by medical science as being necessary and effective steps in combating crippling gender incongruency, which untreated causes sever depression, self surgical attempts, and suicide.
We cry to the heavens for help, please rethink blanketed exclusions of our minority’s necessary health care.
https://www.euro.who.int/en/health-topics/health-determinants/gender/gender-definitions/whoeurope-brief-transgender-health-in-the-context-of-icd-11
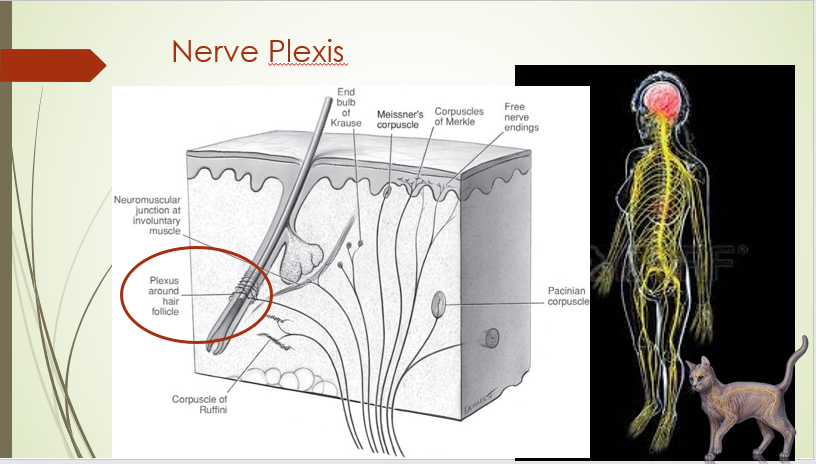
“the nervous system consists of two main areas: central, the brain and spinal cord; and peripheral, the nerves coming from the brain and spinal cord to innervate areas of the body. The control of the nervous system falls into two separate categories: the somatic and autonomic nervous systems. The somatic nervous system relays voluntary (conscious) signals to activate skeletal muscle movement to allow your pet to navigate its surroundings. In contrast, the autonomic nervous system relays involuntary (unconscious) signals to regions of the body to control your pet’s internal organs, such as the lungs, heart, and intestinal tract. skin acts like a glove over your cat’s body providing warmth and protection. Secretions from the skin form a barrier to keep germs and water outside the body and bodily fluids inside. Breakdowns in this protective barrier lead to conditions such as: hair loss, infections, and fluid losses”
https://www.richmondveterinaryhospital.com/client-resources/interactive-animal/species/feline/system/nervous/
BTW kitty has alot more whiskers than you think, there’s a Godzilla trail down the back from tip of the ears to the tail, shoulders, belly and all 4 legs! main mini clusters are center on back of the head, between the shoulders, 3 points on the rear (spine and both flanks), and a couple braids along the tail. Orca’s black an white, bellys white so cant verify location of belly clusters, though he does need a new black kitten freind to teach how to cat :3
“Most cats have eight to 12 whiskers on each side of their nose for a total of 16 to 24 specialized sensory hairs…your feline friend also has whiskers above the eyes, chin, and on the backs of their forelegs? These whiskers are shorter and less noticeable than the ones on thier nose…Because whiskers are so sensitive, pulling on them can cause your cat pain. never trim your kitty’s whiskers…This may cause disorientation, dizziness, and confusion…Unlike ordinary hair, whiskers can sense objects around them. The roots of your cat’s whiskers extend much deeper into the skin than the fur, and a generous supply of blood and nerves feed them. This is how whiskers are sensitive enough to detect a slight change in the breeze. Whiskers come in different lengths for different animals.
https://www.germantownvet.com/blog/cat-whiskers-sensitive/
What is a Root Hair Plexis?- “This bundle of nerves encompasses the bulb, a section of hair that causes it to grow. The root hair plexus is part of the sensory network associated with the integumentary system of the skin. The nerves are near muscle fibers called arrector pili, which are very tiny muscles that allow hairs to stand up straight when the skin gets too cold. The root hair plexus responds to external stimuli at the cellular level the nerves detect movements of the hair shaft, such as when an object gets close to the skin or when wind occurs. the root hair plexus surrounds the follicle and connects to larger nerves in the dermis, or lower layer, of skin. This bundle of nerves is one of three fine touch receptors in the skin, along with Meissner’s corpuscles and Merkel disks. Meissner’s corpuscles and Merkel disks are closer to the boundary between the epidermis and the dermis, whereas root hair plexuses are lower.”
https://www.reference.com/beauty-fashion/root-hair-plexus-44f8c8cbb9da5198
“A plexus is like an electrical junction box, which distributes wires to different parts of a house. In a plexus, nerve fibers from different spinal nerves (which connect the spinal cord to the rest of the body) are sorted. The fibers are recombined so that all fibers going to a specific body part are put together in one nerve. Damage to nerves in the major plexuses causes problems in the arms or legs that these nerves supply.”
https://www.merckmanuals.com/home/brain,-spinal-cord,-and-nerve-disorders/peripheral-nerve-disorders/plexus-disorders
Stress and the Hair follicle: “Skin is richly innervated by sensory nerves that transmit information about the effects caused by environmental stressors to the central nervous system to develop the systemic response of the organism appropriate to its external environment…Hair follicle transition between distinct hair cycle stages is governed by epithelial-mesenchymal interactions between the follicular keratinocytes and dermal papilla fibroblasts….Administration of ACTH into murine telogen skin causes mast cell degranulation and activation of hair growth in resting hair follicles.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1868107/
Seborrheic dermatitis can flare up anytime and is triggered mainly by:
1- Cold, dry weather
2- Stress
3-hormonal changes
4- harsh detergents
5- medicines; psoralen, lithium, interferon
https://www.medicinenet.com/what_triggers_seborrheic_dermatitis/article.htm
“Seborrhea can be a primary or secondary disease. Primary seborrhea is inherited and occurs in breeds such as Persian cats. Secondary seborrhea is more common with the exact cause not always determined. In these cases it is called idiopathic seborrhea. Secondary seborrhea is often related to an underlying medical problem, such as: hormonal imbalances (especially hyperthyroidism), allergies, parasites (internal and external) – fleas, ticks, fungal infections – especially ringworm [which comes from fleas!], dietary abnormalities – poor diets containing low omega-3 fatty acids, environmental factors (temperature, humidity changes), obesity, musculoskeletal disease or pain – the cat is unable to groom itself properly along the back and tail base.”
https://vcahospitals.com/know-your-pet/seborrhea-in-cats
for trans women this explains pre-operative necessity along with a graphic walkthru of vaginoplasty, covering hirsute PCOS therapy, and various other procedural usage.
https://www.sciencedirect.com/topics/medicine-and-dentistry/hair-removal
“The word “lanugo” is derived from the Latin word for wool, “lana”.It is the soft and downy hair that sometimes covers a newborn’s body… Lanugo is the first hair to be produced by fetal hair follicles, and usually appears on your baby around the 5th month of pregnancy… helps vernix caseosa adhere to your baby’s skin. Vernix is a greasy white wax-like substance that covers your baby’s skin while in-utero in order to keep it warm and moisturised. It also helps the baby slip more easily through your cervix..”
https://sg.theasianparent.com/lanugo-hair-newborns/
Stem cells in embryonic skin development, a walkthru of the life of a hair follicle
https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0716-97602012000300003
the entire mechanism of the fillosebasceous unit consists of 3 areas, the hair itself, the sebasceous glands, and the ductal linning cells aka sebasceous fillaments– (that look like white worms squeezed out your nose)
https://plasticsurgerykey.com/the-folliculopilosebaceous-unit-the-normal-fpsu/
how to get rid of sebasceous fillaments– Dr Bray
fillaments are tubular hair like structures in the pore that bring oil up to the skin, almost like a candle wick..for people with oily skin that can get backed up, and present extruding from the skin as a white dot.. the size depends on three factors; genetics, size of gland, and influenced by hormones.
1-do not squeeze the fillament out as it causes inflammation and scarring, while doing nothing to improve the circumstances…may look like a small white primordial hair when you do.
2-wash your face first thing in the morning..dont overwash, super hot water or agressively overtreat and dry out your skin.. salycidic acid cleanser or “leave on” can decrease the size of the fillament.. Loreal created a LHA thats milder and works the same as salycilic acid..
3-vitamin A retinoid(active state)/retinol(skin must go thru a process to use) decreases the amount of oil and size of the oil gland..
4-clay masks absorbe excess oil from skin an a little from the pore..
5-sunscreen, as UV rays destroys the architecture around the pore making them larger over time.
6-diet, some things increase hormonal growth factors that in turn lead to overproduction of oil. eat fruits and vegetables, oily processed foods are horrible for skin.
https://www.youtube.com/watch?v=pg8w3YngT6I
pubarche, “There is little if any difference in the capacity of male and female bodies to grow hair in response to androgens. The obvious sex-dimorphic difference in hair distribution in men and women is primarily a result of differences in the levels of androgen reached as maturity occurs.
“Pubic hair and axillary (armpit) hair can vary in color considerably from the hair of the scalp. In most people it is darker, although it can also be lighter. In most cases it is most similar in color to the eyebrows of the individual. As with axillary (armpit) hair, pubic hair is associated with a concentration of sebaceous glands in the area.”
https://en.wikipedia.org/wiki/Pubic_hair
^ “The acuminate or “masculine” type is present in approximately half of the men and 10 percent of the women. It is characteristic of 39.8 per cent of 19-20 years old males, and persists in 20.2 per cent of adult males. In the majority the division into “masculine” and “feminine” types is found to be satisfactory. “
https://www.ncbi.nlm.nih.gov/pubmed/3190177
addressing PCOS as an electrologist to a client that doesnt yet know their a patient, hirsutism vs hypertrichosis, “it is the free angrogens in the blood the bodies not currently using from overproduction, along with follicles that have predisposed genetic sensitivity too stimulation…check for signs of dark growth not only on the the upper lip and chin area but on cheeks, forearms, hands, back of the neck, center and top of chest (women naturaly have 30 or so hairs on each breast, center is masculine pattern)..it is imperative that we screen clients for possible hormonal issues that they may not be aware of nor yet brought to their physicians attention…while it will cost you the income those extended sessions it will save you sleep at night knowing your client is in good hands.“- Dianne M. Roling
https://professionalelectrolysisservices.com/video-presentations/
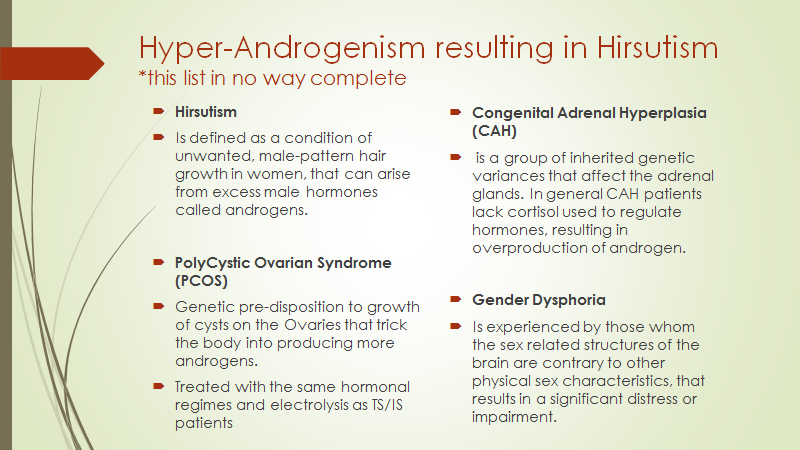
“Hirsutism is defined as the presence of terminal hairs on women in a male-like pattern and often is a sign of underlying androgen excess (hyperandrogenism)
“Therapy for the patient with unwanted hair growth would not be complete without treatment to remove existing hair growth (Table 3). A number of methods have been reported to reduce unwanted terminal hair growth, including electrology and laser hair reduction. Electrology has been available for decades, and although prospective randomized trials are few, extensive clinical experience appears to indicate that it does afford permanent hair reduction in most patients. Laser hair reduction is a much newer modality, and although it does appear to offer less-permanent hair removal than electrology it provides significant hair reduction. Nonetheless, these methods do have their drawbacks. Electrology requires multiple and frequent treatment sessions that can be painful, depending on the location and extent of hair involvement. Likewise, laser hair removal has the potential for causing skin damage and is primarily effective in those patients who have dark hairs and lighter skin. Both of these methods can be quite costly in the long run. As such, the recent advent of newer topical therapies for reducing hair growth is of importance.”
Conclusion
More than 14 million women complain of unwanted facial hair growth, approximately one fourth of whom actually suffer from hirsutism. Evaluation of these patients should include a determination of whether they actually have hirsutism and have concomitant endocrine or metabolic abnormalities. The appropriate treatment for a woman who has unwanted hair growth may include hormonal therapy, but should also include mechanical and/or cosmetic means of removing hair growth. The newly approved eflomithine HCl cream, 13.9% is a useful adjuvant in reducing noticeable hair growth in affected women.
http://www.soulcysters.net/showthread.php/7019-Advances-in-the-evaluation-and-treatment-of-unwanted-hair-growth-(PCOS-mentioned)
Hirsutism is an excessive body and facial hair growth in women in locations where is normally minimal or absent following a hair-male pattern. For this reason is not uncommon that hirsutism raises psychological, cosmetic and social concerns. There are many treatment modalities that can be summarized into two broad groups: pharmacologic and non-pharmacologic treatment. Until now, medical treatment has been designed to interfere with the synthesis of androgen at the ovarian or adrenal level, or inhibit the effect of androgen at the receptor level, although recent progresses test other options such as insulin modulators or ornithine decarboxylase inhibitors. Mechanical treatment includes laser hair removal, electrolysis, depilatory creams, plucking and waxing. This article presents a general overview of hirsutism treatment options.
http://www.ncbi.nlm.nih.gov/pubmed/20218823
commonly refered to as “werewolf syndrome” hypertrichosis is the term used to denote excessive and abnormal growth of hair, on any part of the body which is more than is seen in individuals of the same sex, age, and race as the person under consideration. Genetic, or acquired, androgen-independent excessive hair growth. The two distinct types of hypertrichosis are generalized hypertrichosis, which occurs over the entire body, and the more common Localized hypertrichosis, which is restricted to a certain area.
http://emedicalhub.com/hypertrichosis/
“Facial hypertrichosis and hirsutism may cause severe cosmetic and psychologic problems. In the following, new developments in the treatment of hypertrichosis will be presented. Permanent depilation by photothermolysis is currently the most promising treatment. A new topical treatment of hypertrichosis is eflornithine cream. It inhibits the enzyme ornithine decarboxylase which is essential for the rapidly dividing cells of the hair follicle. Furthermore, other methods of hair removal such as plucking, waxing, chemical depilation by thioglycolates, electrolysis, thermolysis and systemic therapies of hirsutism will be discussed.”
http://www.ncbi.nlm.nih.gov/pubmed/11757465
“Hidradenitis suppurativa most commonly occurs in women between the ages of 20 and 30. The ratio of female to male is three to one. There is some research that shows HS is a disease of hair follicles that has genetic and environmental causes..With heat, the pore can get clogged and a cyst will form, holding a collection of fluid, within a closed area..bacteria then accumulates in this environment and eventually the cyst ruptures and causes inflammation. Most of us will get ingrown hair, but people with HS are prone to chronic inflammation and recurring boils, which are painful and cause scarring. HS is not caused by poor hygiene, nor is it a sexually transmitted disease or contagious. important that patients recognize triggers that can cause flare-ups, such as wearing tight clothing, shaving, smoking and gaining weight,There’s no cure for HS, so you’ll have to manage the condition for life.“
https://www.huffingtonpost.ca/2018/07/31/hidradenitis-suppurativa-skin-condition_a_23493257/
Trichotillomania is the obsessive plucking or ripping of hair from the head, face, hands, genital, body
http://www.ocdonline.com/#!trichotilomania/cauz
^ awesome resource for Body Focused Repetitve Behaviors, the TLC Foundation
http://www.bfrb.org/index.php
^How to get insurance to pay for your BFRB treatment
http://www.wsps.info/index.php?option=com_content&view=article&id=94:fight-for-your-rights-getting-insurance-to-pay-for-your-treatment&catid=0
Polycystic Ovary Syndrome and intersex
http://feministing.com/2009/07/23/pcos-and-intersex/
“how many trans people are there in America? 1.4 million, expect that to increase as they include us in census and allow human rights, a lot are fearfull, thus closeted
http://www.lgbtqnation.com/2016/06/estimated-population-transgender-americans-doubles-1-4-million/
how many trans people are in your state? Ohio has .45% or less than half of 1 percent
http://fusion.net/story/321184/how-many-transgender-are-in-us/?utm
preliminary UCLA law statistics
http://williamsinstitute.law.ucla.edu/visualization/lgbt-stats/?topic=LGBT&area=39#density
how many are born intersex? 1/150
http://intersexroadshow.blogspot.com/2012/03/how-common-is-intersex-status.html
Twice as many children want gender treatment than expected in Denmark
http://www.gaystarnews.com/article/denmark-copenhagen-gender-clinic/#gs.hnF1TdA
CDC study finds 2% of grade-school students identify as transgender
https://www.washingtonpost.com/education/2019/01/24/cdc-nearly-percent-high-school-students-identify-transgender-more-than-one-third-them-attempt-suicide
“What is the minimum number of people in group required for you to treat them with respect? How many is too few? How many is enough? Do we really only need to treat people with respect when there are enough of them?”
http://www.thenewcivilrightsmovement.com/rjmedwed/what_s_your_answer_to_why_should_i_care
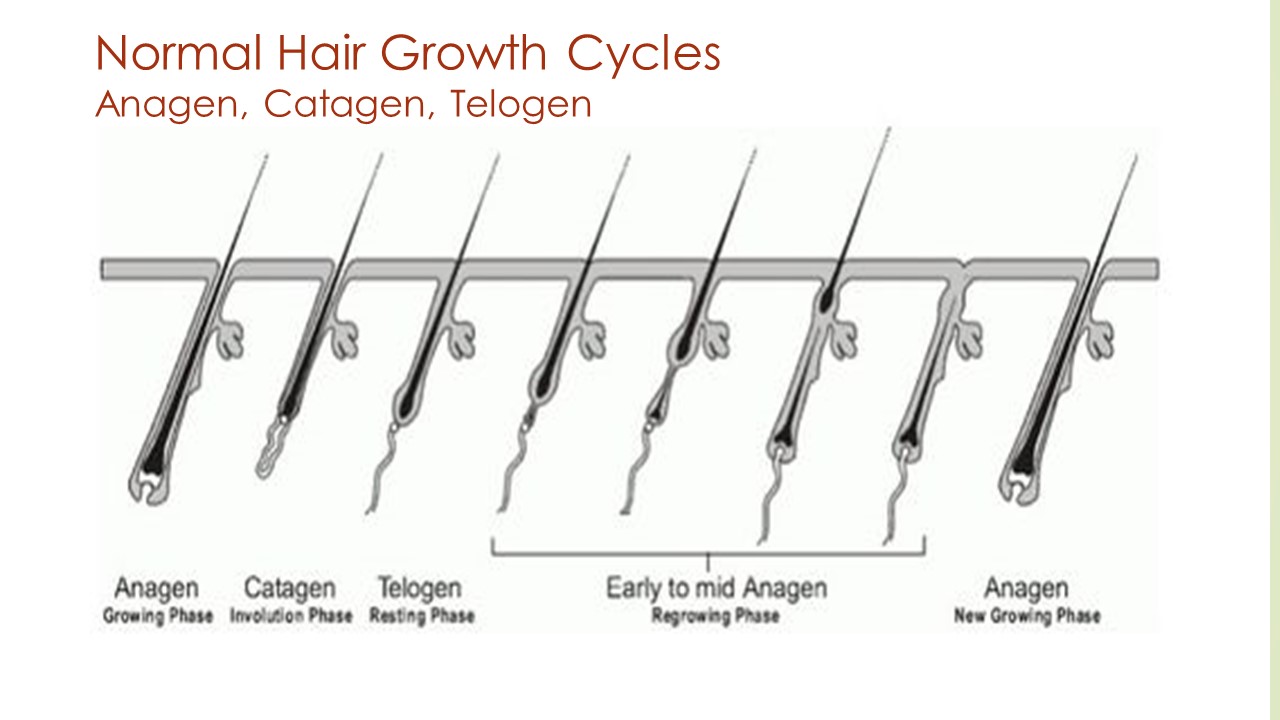
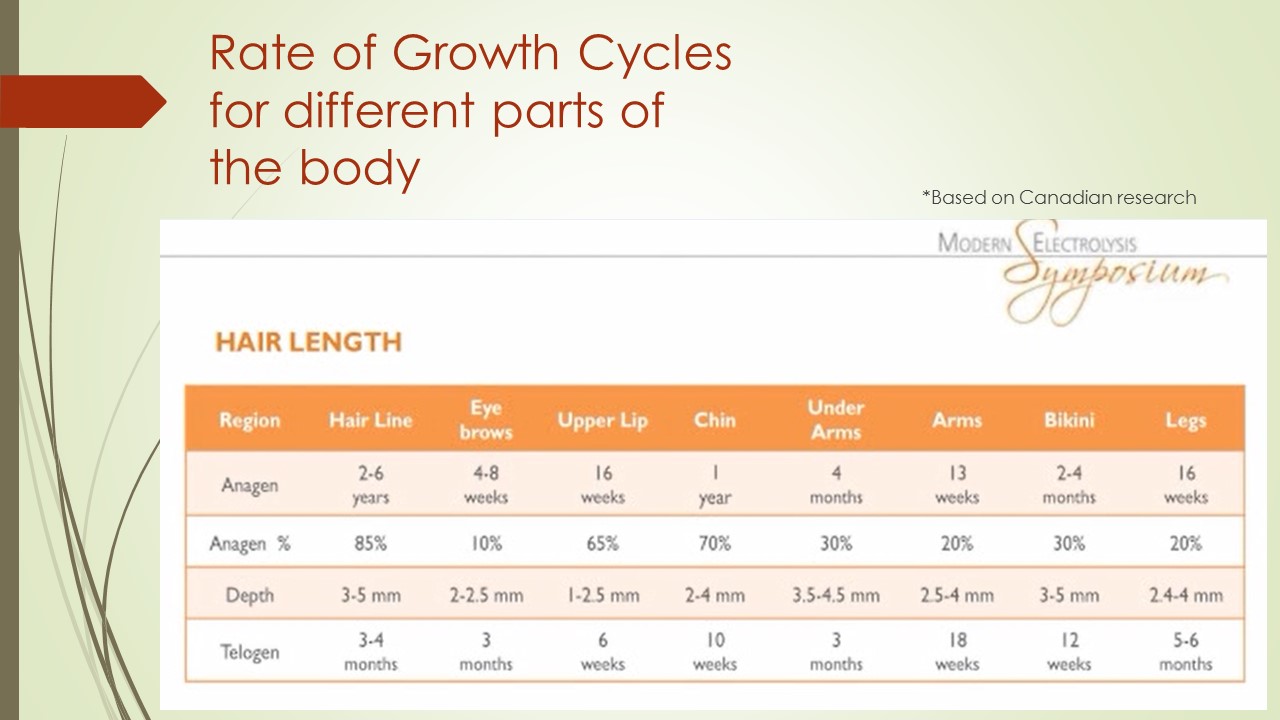
Think of hair follicles as a fillosebasceous unit consisting of the hair<sebasceous glands<and the hair matrix; only 25% is in an active growth cycle so look at these as popcorn in the microwave going off< what caused that is a chemical cascade that fluctuates with the level of androgens in your blood, which can cause them to “pop”/grow at higher or lower rates.
The permanent removal of hair must be done to the entire genital region before surgery, conservative timing, that is if i could afford to go to an electrologist once a week, for an hr, sets one back at the very least a yr before we can even schedule surgery. they say a yr generally, because hair grows back in stages. true regrowth from treatment itself comes back as strong, meaning sometimes having to treat a follicle multiple times. and then theres the new cyclical growth from previously dormant pores also needs to be rid of, “having sex with hair growing from the inside of your vagina will not be comfortable in the least”. so like those of remedial means back to hopelessness, as one cannot afford weekly treatments of electrolysis needed to make that timeline in the forseeable future. i cant even rid my face of these dirty stitches, let alone start and finish in an “unnoticeable” area. though it plagues me an i can feel anagen growth weeks before any visible hair thru yrs of plucking the area which has only made the hairs thicker and deeper. the cheapest electrolysis one can find is $65 an hr, thats impossible to pay somone a dollar a minute when you dont even make a dollar an hr. i dunno, about to start doing my own procedures, meaning electrolysis , with no teacher or mentorship. as that seems to be my only option.
walk thru of the functions and stages of a hair follicle; Anagen, Cantegen, Telogen
https://en.wikipedia.org/wiki/Hair_follicle
some claim “early Anagen” as a 4th cycle called Exogen, but this has yet to be proven as a distinct hair phase outside of the scalp tissue in humans, and of more importance to regrowth than removal (though how cool would it be to not only remove but replace hair lost to alopecia!). Theorizing this would be due to the length of the growth cycle on the head lasting yrs as opposed to months on the arm.
https://www.ncbi.nlm.nih.gov/pubmed/17908196
“Kyocera, along with RIKEN and Organ Technologies, has launched a joint research to develop a regenerative medical treatment for hair loss, targeting practical use in 2020. The joint research works on a technology to collect stem cells from the patient’s own hair follicles, followed by the processing of these follicles and autografting on the same patient. For the treatment of androgenic alopecia (the most common type), a small number of hair follicles will be collected, from which stem cells will be isolated, cultured and amplified to produce hair follicle germ. The regenerated hair follicle germ will be packaged and delivered to a medical facility for use in transplantation therapy for the patient. The method furthermore allows control of the hair color by adding pigment stem cells, and the number of hair follicles regenerated.”
https://uk.kyocera.com/index/news/previous_news/news_archive_detail.L2NvcnBvcmF0ZS9uZXdzLzIwMTYvS3lvY2VyYV9fYWxvbmdfd2l0aF9SSUtFTl9hbmRfT3JnYW5fVGVjaG5vbG9naWVzX19oYXNfbGF1bmNoZWRfYV9qb2ludF9yZXNlYXJjaF90b19kZXZlbG9wX2FfcmVnZW5lcmF0aXZlX21lZGljYWxfdHJlYXRtZW50X2Zvcl9oYWlyX2xvc3M~.html
if your a potential investor here is something you…
* bet theres a market for hair stem cells in research if you could meet their standards for acquisition. i mean your already in there, why cant we just scrape out stem cells and leave a healthy (perhaps weakened) follicle in people without hair issues- like a plasma center. you can then scrub and cascade em’ to work in equivalent body types/areas (stem cells can become any cells). this would then become something anyone with hair issues could initially go to on their own, to perhaps assist or even afford the electrologist. But like anything bigots will ruin it, first we need to overturn exclusions on LGBTI people in current centers.
-“James began donating plasma to the center located in Duluth in 2011. The center required her to list her assigned sex at birth on the intake form. As she continued to donate plasma, James began marking female on the form, consistent with her gender identity. In June 2015, an employee informed James that CSL Plasma did not permit transgender persons to donate plasma and prohibited her from donating. In February 2016, James filed a charge of discrimination with the Department of Human Rights and the department investigated the allegations. The lawsuit goes on to say in November 2017, the department found probable cause that CSL Plasma allegedly discriminated against James because of her gender identity. The plasma collection center refused to settle the case through the department’s conciliation process. CSL Plasma would continue to discriminate against James, as in October 2018, they again denied her the ability to donate at a collection center in Minneapolis.
https://kstp.com/news/csl-plasma-sued-for-discriminating-against-transgender-woman-/5271198/
^”While this lawsuit was pending, the U.S. Food and Drug Administration (FDA) updated its blood donor recommendations in 2015…the updated guidance provides a clearer position on transgender donors. Donation centers are now advised that they should accept a donor’s own identification of their gender. And as we have argued all along, the FDA’s updated guidance continues to provide no ban on donations based on the fact that a person is transgender. “
https://www.redcrossblood.org/donate-blood/how-to-donate/eligibility-requirements/lgbtq-donors.html
old patent from 1974, for a hypodermic needle meant to deposit chemicals inside the follicle for depilation.
Patent 3794028 – METHOD FOR INJECTING CHEMICALS INTO THE PAPILLA FOR DEPILATION
https://patentimages.storage.googleapis.com/05/51/b1/4ee01aa556877c/US3794028.pdf
those chemicals could be specified to release the stem cells, and simply plunge the created slurry back out. then spin it into its constitute parts.
using a centerfuge which works based on molecular weight: every atom of every molecule that adds up to create any ion has a specific weight based on its composition. Centrifugal force throws it apart at the same time gravity pulls it back in, as seen in the rings of Saturn.
http://adsabs.harvard.edu/full/1966MNRAS.133..247Y
“Separation is achieved by spinning a vessel containing material at high speed; the centrifugal force pushes heavier materials to the outside of the vessel. This apparatus is found in most laboratories from academic to clinical to research and used to purify cells, subcellular organelles, viruses, proteins, and nucleic acids. There are multiple types of centrifuge, which can be classified by intended use or by rotor design… used for applications like quick production of PPP (platelet poor plasma) and PRP (platelet rich plasma) as well as the separation of serum, urea, blood samples and other routine applications in hospital and research laboratories. Look for certifications if your lab has requirements for invitro diagnostic (IVD) medical equipment. Optional adapters are available to accommodate various tube sizes including standard conical tubes and round bottom blood tubes. Units are available that include features for cell culture processing, blood sample preparation, and microplate applications. “
https://www.biocompare.com/Lab-Equipment/Laboratory-Centrifuges/
concept consists of:
1-making the client overproduce sebum, which itself has some stem cells in and around the sebaceous glands,
2-using sonophoresis to bypass the horney outer layer
“Low‐frequency ultrasound (20 kHz) has been found to be more potent in enhancing skin permeability than therapeutic ultrasound (1–3 MHz)”
https://onlinelibrary.wiley.com/doi/full/10.1211/jpp.61.06.0001
3-in conjunction with a topical ointment that after dispursing its toxicologic components, should then secoundarily mix in well with sebum; and have a higher acclamation rate specific to the stem cells greater than those forces keeping the stem cells in the bulge region, wicked in the filaments, or suspended in sebum.
4-apply a occlusive plastic sheeting, let the area become inflamed and locally seborrheic as it starts sweating out your gold.
5-apply suction to the sheeting gathering your slurry, followed by microneedling to gather the trapped sebum (which will create its own layer in the skin between the epidermis and dermis (similar to oil in depths of the earths crust)
6- spin it all until you’ve panned your gold,
7- package store and disseminate.
need investors and research buddies! 5-26-21
^they do a “modern electrolysis symposium” in Quebec Canada, this is 2015’s. Dectro International hosts it every year. They produce the Apilus machines
http://www.electrolysissymposium.com
Summary of Hair Removal Methods
| METHOD | SIDE EFFECTS | PERMANENCE | COST |
|---|---|---|---|
|
Shaving |
Chemical dermatitis, minor cuts, pseudofolliculitis barbae |
One to three days |
Variably inexpensive |
|
Epilation: plucking/waxing |
Pain, folliculitis, pseudofolliculitis, burns, irritation, postinflammatory hyperpigmentation, scarring |
Two to eight weeks |
Least expensive |
|
Depilation: chemical |
Chemical dermatitis, occasionally allergic dermatitis |
Up to two weeks |
Variably inexpensive |
|
Laser |
Edema, erythema, pain, hypopigmentation, hyperpigmentation |
At least three months |
Variable but approximately six to eight sessions (depending on site and skin/hair color), at $75 to $250 per session |
|
Electrolysis |
Edema, erythema, pain, scarring, keloid formation, postinflammatory pigment changes. Cannot be used by patients with pacemakers. |
Considered to be permanent but depends on method and operator |
About $18 to $25 per 15-minute session; variable number of sessions initially, followed by maintenance |
|
Topical: eflornithine, (Vaniqa) |
Acne, pseudofolliculitis barbae stinging, burning |
Up to eight weeks after discontinuing treatment |
Approximately $50* for one month of twice-daily treatment |
^
https://www.aafp.org/afp/2002/1115/p1907.html
From Flint Rocks to Lasers, a History of Hair Removal Methods (awesome resource highly recommended reading)
https://www.ncbi.nlm.nih.gov/pubmed/23725310
razing/shaving
personally suggest doing this in the shower
warm water will swell and soften the hair before you raze, it also opens the follicle which allows it to extend further for a closer cut=smoother shave.
cool water immediately after razing will close the follicles and pores protecting them from bacteria.
https://share.upmc.com/2018/11/how-to-get-rid-of-razor-bumps/
Benzoyle peroxide topical wash can help speed up the release of in-growns (have your dermatologist prescribe its covered)
https://www.youtube.com/watch?v=MyPm5CUfEOU&feature=youtu.be
 a Venus handle fits a Mach3 blade. built these kits too give other trans peeps, understand that the most marginalized of us never really had anyone teach us proper self care or have the means to financially sustain it. right now the kits go to people who need them met in my adventures; facing societal barriers like streets an shelters. people who have lost everything, who may or may not have access to healthcare or afford the basic necessity’s, let alone medical necessity’s, or a decent razor. used to be one of them, still am, keep a kit in passenger door.. no help or connection with P@G (tried), simply like the product.
a Venus handle fits a Mach3 blade. built these kits too give other trans peeps, understand that the most marginalized of us never really had anyone teach us proper self care or have the means to financially sustain it. right now the kits go to people who need them met in my adventures; facing societal barriers like streets an shelters. people who have lost everything, who may or may not have access to healthcare or afford the basic necessity’s, let alone medical necessity’s, or a decent razor. used to be one of them, still am, keep a kit in passenger door.. no help or connection with P@G (tried), simply like the product.
psuedofolliculitus<folliculitus barbae<sycosis barbae<keloids
https://www.youtube.com/watch?v=zB5ESIXsGdw&feature=emb_logo
folliculitus barbae is a foreign-body inflammatory reaction surrounding ingrown hairs. It can also occur on any body site where hair is shaved or plucked. Folliculitis barbae and pseudofolliculitis barbae can co-exist. Pseudofolliculitis barbae presents as ingrown hairs associated with flesh-coloured or red follicular papules, which may be itchy or tender. Folliculitis barbae presents as painful pustules and can discharge pus.
- the current suggestion is wait 30 days before you shave again to give ingrowns time to release.
- Ensure the skin is well moisturized, for example using a lotion containing glycolic acid to the affected areas. This exfoliates the surface skin cells and reduces the likelihood of new inflamed spots.
- before shaving cleanse the skin using a polyester skin-cleansing pad or a moisturizing shaving foam.
- Aim to have a 5 o’clock shadow immediately after shaving. Shave less frequently, eg every other day. [imagine being a woman with this]
- Either use a single blade disposable razor or use electric hair clippers or a razor with an attachment that leaves the cut hairs long.
- Shave in the direction of the follicle, not against it. Do not stretch the skin.
- Sterilize metal hair clippers and electric razors using boiling water, and plastic items should be soaked in an antiseptic solution.
- To prevent recurrence follow a proper shaving regime and consider permanent hair removal options. Laser hair removal, especially Nd:YAG and diode lasers, have been shown to be beneficial but there is a risk of causing white or dark marks in skin of color.
https://dermnetnz.org/topics/folliculitis-barbae/
“Pseudofolliculitis barbae affects around 45% of African American Service Members, a lower percentage of Hispanics and about 3% of Caucasians.3,4…cases often warrant restrictions on shaving or laser therapy.“
https://academic.oup.com/milmed/article/186/1-2/e52/5948064
“can occur as a complication of shaving in men or women from any racial and ethnic group..This approach is appropriate in all women, but Dr. Roberts focused on her experience with black patients..
- for whom an antioxidant cream is added to address the inflammatory-associated hyperpigmentation that often accompanies..
- Start with microdermabrasion to treat the hypertrophic hair follicles and address keratin plugs. The microdermabrasion smooths the skin and increases penetration of subsequent creams and topics.
- In the same session, I treat with Nd-YAG 1064 nm laser using short pulses,” she noted. For black women, she makes four passes with the laser at a level of moderate intensity. For those with lighter skin, she might perform as many as six passes with the laser set higher. The microdermabrasion is repeated monthly for three or four treatments, but can be extended for those with persistent symptoms
- over the course of treatment nightly topical tretinoin is recommended for maintenance. Regular use of emollients is also recommended. For black women who have developed hyperpigmentation as a complication of pseudofolliculitis barbae, prescribe a lightening cream.
https://www.mdedge.com/dermatology/article/209883/aesthetic-dermatology/combined-treatments-provide-control
“regulations in the U.S. military have found us sacrificing our skin by shaving over fibrotic tissue, ingrown hair, and bumps, only to leave our faces looking like a battlefield...a mentor advised me to consider the stigma associated with having a shaving profile. I was told to look at people in officer leadership roles and consider how few of them had shaving waivers. I then began to see the realities of having the waiver and what it meant to me in my future transition to the officer corps…Having to repeatedly renew a waiver for a chronic condition systematically drains time away from duties, an obstacle that our colleagues do not similarly experience…was given the option to undergo laser treatment. But during the informed consent, the trade-off that I had to weigh was being able to grow a dense and healthy beard versus giving it up to adhere to military requirements. Or, in the future, after I leave the military, if I want to grow a beard, will I be unpleasantly surprised by traumatized hair follicles that produce thin, patchy, and sparse hair growth?
https://academic.oup.com/milmed/article/186/5-6/143/6131712
Double-edged razor blades have been associated with transfollicular penetration of growing hairs. When using multiple blade razors, the first blade pulls the hair while the second cuts the hair…The pulled hair retracts into the follicle giving a smooth shave but encourages transfollicular penetration..Stretching the skin before shaving, shaving against the grain or use of blunt blades may also increase the chance…increasing the frequency of shaving can reduce the occurrence of PFB…
Pre-shave regime, especially with warm water causes the hair shaft to swell thus reducing the chance of producing a beveled, sharp tip
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6585396/
a nice video done by Andrew Vardanian, MD UCLA, that explains keloid scarring and its treatment options, this is what happens to people living with Pseudofolliculitis barbae 😦
https://www.youtube.com/watch?v=rJSnC2pHoJ4&feature=youtu.be
single blade safety razors are needed for those who tend to get razorbumps. plus side is they will save $$ on blades in the longrun.
https://www.youtube.com/watch?v=eJvWGJRKD58
let the weight of the razor do the cutting, safety razors are a different experience than multiblade
https://shave.net/blogs/shaving/shave-your-legs-with-a-safety-razor
pink butterfly one! parker has a nice selection of cool handles (butterfly is a handle that opens at the turn of an end to replace blades, as opposed to the vintage 3 piece)
https://www.parkershaving.com/c/parker-razors/safety-razors/
hair trimmers are what you need to learn to use “down there” in preparation for permanent hair removal treatment, to cut down on ingrowns and barbae- “stop plucking, stop razing, use the trimmer guard!”- Dr. Kerrith Spiknall
it takes about 5 days for your hair to grow long enough so its not longer stabby, which matches the 5mill guard attachment.
then ironically, we may ask you to shave 3-5 days before treatment (if you are able too), because the anagen hairs will be more noticable/longer than the telegen, allowing the technician a higher kill rate by treating during the most optimal time.
https://www.electrolysisbeautylounge.com/before-during-after
on the flipside, the telegen hairs will be the longer hairs for hair that is in an all-natural state. meaning not recently razed or waxed, having all hair stages going on at once.
“over treatment of the eyebrows and upper lip can occure by letting the patients self image pressure you into treating vellus hairs that are about to fall out. its always, “just the long ones”.”- Mike Bono
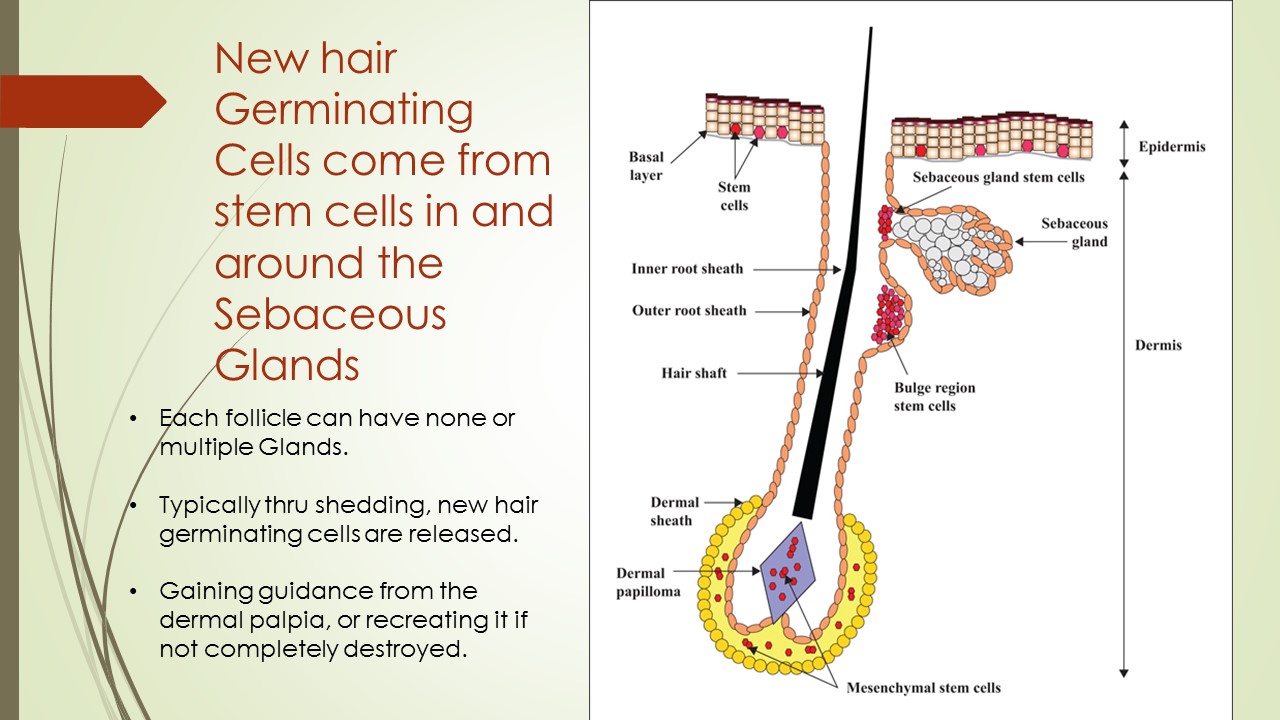
^ this graph shows the importance of destroying not just the root of the hair but as much of the lower 2/3rds of the follicle as possible
stem cells of the skin and their lineages
http://lab.rockefeller.edu/fuchs/research/stem
Dissecting the Bulge in Hair regeneration
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3266778/
Bulge region as a Putative hair Follicle Stem Cell Niche
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5632317/
![20210101_000327[1]](https://kittysbelle.files.wordpress.com/2015/10/20210101_0003271.jpg)
 pili multigemini (two or more hairs from a single follicle) trapped hairs cause the circular growth.
pili multigemini (two or more hairs from a single follicle) trapped hairs cause the circular growth.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4830170/
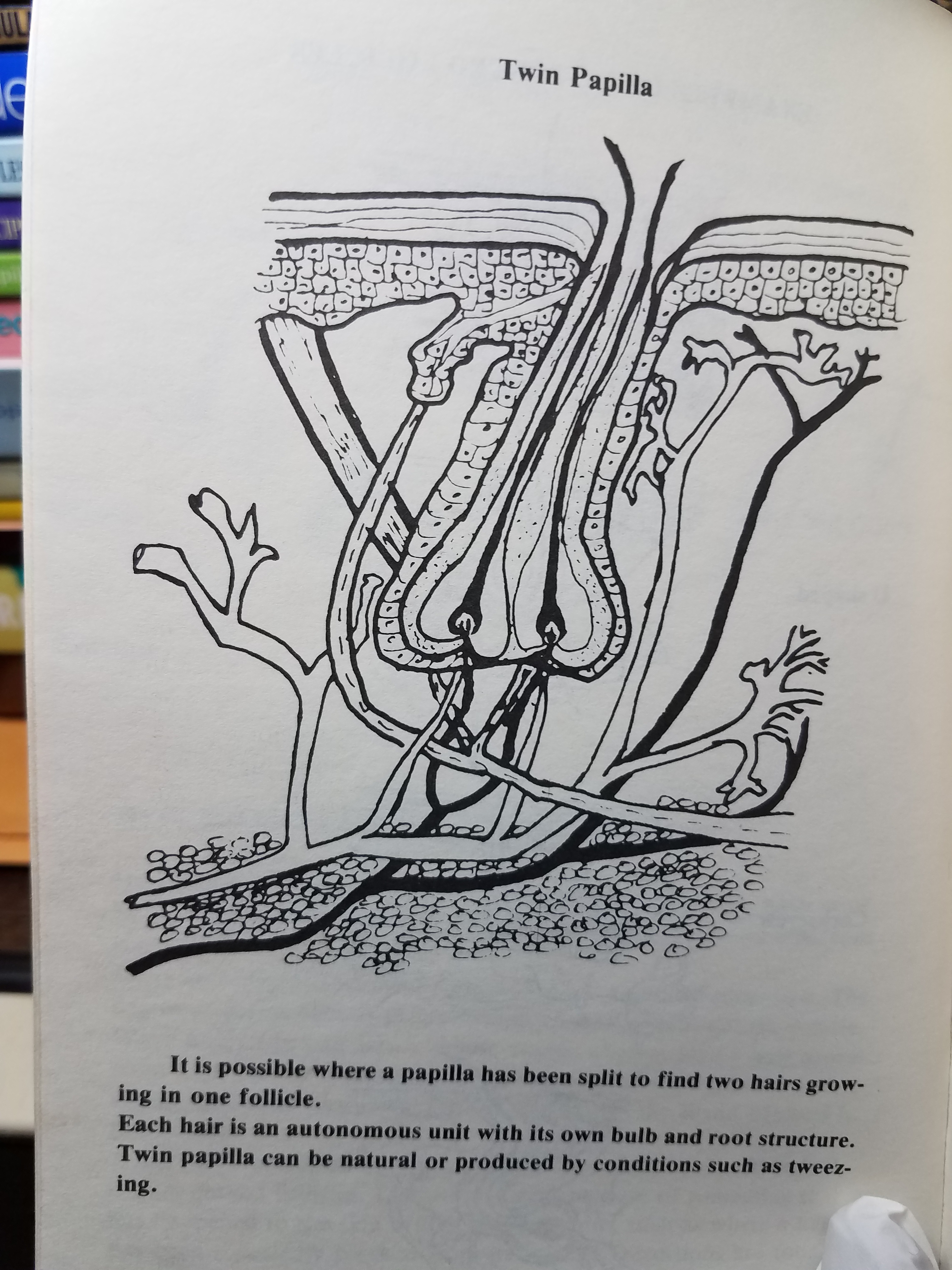
image of twin follicle, Electrolysis and You, Ali Baysinger+Lois Ulmer- quit plucking!
http://booksnu.info/doc/electrolysis-and-you-permanent-hair-removal-paperback-by-baysinger-m-ali
every time you pluck a hair it takes approximately 13 weeks for that hair to grow again
https://allbodieswelcome.com/f/why-is-plucking-so-bad
“When treating PMG follicles I generally apply slightly higher treatment energy via timing, intensity or pulsing. To improve comfort, I use the largest needle that will fit in the follicle without dimpling the skin during insertion. Sometimes I will apply current at three separate locations like treating the bottom corners or a pyramid. Treating multiple times at different depths is also a viable option. Each hair in a pili-multigemini cluster will have its own cycle, unrelated to adjacent hairs.“-hairadicator
https://hairtell.com/forum/t/diyers-areas-goals-concerns-and-progress/38767/48

how long will electrolysis take? Est 200hrs but can be from 1-400
http://www.tsroadmap.com/physical/hair/zaptime.html
A full, thick beard will likely require 3 – 6 hours of treatment each week for up to 5 years to finally achieve permanently smooth skin. Although the treatment time will gradually decrease, this still represents a huge time commitment. As for cost, it is unlikely to end up being less than $10,000 and could be considerably more.
Https://hairfreelife.com/different-types-electrolysis-best/
genital work- “Generally speaking, you are likely to require treatment for at least 12 months. It can take anything from 8 months up to 2 years in some cases. we strongly advise electrolysis before the operation because laser is not always permanent, and after the operation you won’t get a second chance”
https://2pass.clinic/en/hair-removal/procedures/genital-electrolysis
“When you start hair removal, about 25% of the hair follicles will be in the active stage, while others will be in the transitional and resting phases. Only the hairs in the active phase will be affected by electrolysis or LHR. Many surgeons recommend planning for 6-12 months of hair removal, followed by a wait time of 3 months to confirm that regrowth won’t occur.”
https://www.mtfsurgery.net/vaginoplasty-hair-removal-guide.htm
choosing an electrologist, understanding hair growth, treatment, pain, dangers
http://www.transgendercare.com/electrolysis/index.htm
“The US Food and Drug Administration (FDA) is recommending patients and caregivers keep cell phones and smart watches at least 6 inches away from implanted medical devices, such as pacemakers and defibrillators…recent research reporting that high field strength magnets in newer smartphones may cause some implanted medical devices to switch to “magnet mode” and suspend normal lifesaving operations.”
https://www.medscape.com/viewarticle/951089
if you feel plucking your treatments are not effective and the hairs will grow back, the hair should slide out with little to no resistance.
https://www.youtube.com/watch?v=vQ5Gk7qP4DU
“what are those black dots after electrolysis?”
tombstones, are early anagen stage hairs underneath of the hair visible and treated that was actually in late telogen, and youve successfully cut off the blood supply to the area, meaning that new hair underneath it (that would eventually push the old out and replace it), died and is working its way back up like a splinter (though it has a follicle opening so no worries). it also happens when a hair is severed and not fully removed during treatment.*though can become embedded in scar tissue from improper treatment
https://www.follikill.com/2014/02/27/black-dots-after-electrolysis/
It can vary up to a year in some cases to know if scarring occurs. The leaing plasma ( yellowish fluid) is a cause for concern and would indicate excessive current was used, but it’s unlikely the treatment will result in any permanent scarring, In any event if it were to do so, we generally would not know this until at least 9 months or more has passed.
https://hairtell.com/forum/t/help-scars-from-electrolysis/53614/8
Baghdad battery, 250 BCE, using vinegar, or any other electrolytic solution – the jar produces about 1.1 volts (.001ma)
https://www.smith.edu/hsc/museum/ancient_inventions/battery2.html
“Electrolysis is not a new technology. It was re-discovered in 1800 by William Nicholson and Anthony Carlisle, using voltaic current. The invention has an interesting story: It was a few weeks after Alessandro Volta revealed his invention of the voltaic pile that William and Anthony decided to replicate Volta’s experiment. In brief, during the experiment they accidentally contacted wires with water and observed some gases, which were found to be hydrogen and oxygen. This led to the birth of the new science, “electrochemistry” [27]. https://www.sciencedirect.com/topics/earth-and-planetary-sciences/electrolysis#:~:text=Electrolysis%20is%20not%20a%20new,decided%20to%20replicate%20Volta’s%20experiment.
1800-1920 is considered the age of “quack” experimentation with electrical variation; Polysene, Sinusodal, Wave currents,etc
http://www.electrotherapymuseum.com/Museum18001900_Magneto_Electric.htm
“It wasn’t until 1875 that electrolysis [was applied to hair removal]. Dr. Charles Michel, a St. Louis ophthalmologist, devised this system to remove his patients’ painful ingrown eyelashes.” https://www.cranstonelectrolysis.com/page/page/3379868.htm
“At first, the hair was removed before the follicle was destroyed but, in 1882(1869?), the dermatologist Charles Henry Fox began practicing electrolysis with the needle introduced alongside the hair (Colwell, 1922, p. 89), the practice commonly employed to this day.”
https://www.cosmeticsandskin.com/bcb/electrolysis.php#:~:text=At%20first%2C%20the%20hair%20was,commonly%20employed%20to%20this%20day.
using Kromayers needles in 1908-1916
https://www.cosmeticsandskin.com/bcb/electrolysis.php
the following 6 books cover galvanic as used for hair removal through the age of “quack”, so its from the time of ingenious violet wand hair combs and electric bathtubs, yet galvanic electrolysis survived as a true medical use.![20210314_133006[1]](https://kittysbelle.files.wordpress.com/2015/10/20210314_1330061.jpg) 1-Treatise on Electrolysis and Its Applications to Therapeutical & Surgical Treatment in Disease. Wood’s Library of Standard Medical Authors, Amory, Robert, 1886. 1st Edition.
1-Treatise on Electrolysis and Its Applications to Therapeutical & Surgical Treatment in Disease. Wood’s Library of Standard Medical Authors, Amory, Robert, 1886. 1st Edition.
2-The Electro Therapeutic Guide ~ William Howe ~ 1902
3-“MEDICAL ELECTRICITY At Home” Tradewell, 1904
4- Electricity and the Methods of its employment in removing Superfluous Hair and other Facial Blemishes;- Plym S. Hayes MD, 1910 c1880
“I will remember the unfreindly criticism of some members of the medical profession who had less knowledge of the physics and theraputics of electricity than they have of some other branches of medical science. That time has passed. So many have proven the competancy of the process that if failure is recorded, the operator not the method is to blame. During the years of use in removal of superfluous hair, i have come across all grades of difficulty, drawing on my experiences and modifications of the operation to which they can be overcome.”- Hayes
5- archives of electrology from 1923, vol3 *
“Electric vibrations differ from other forms of vibration only in rate and number. We have different kinds of light vibrations, not only considered qualitatively but also quantitatively, and we may consider electric vibrations in the same way. The simplest form of electric vibration is the direct (DC) or continuous current-commonly called galvanic electricity. Next we have the alternating or indirect current-commonly called Faradic electricity. The particular use of the direct current is to produce chemical changes. This property is due to the fact that this current always moves in one direction. The indirect current is purely a function regulator, due to its to and fro motion, (which excites the medium and produces heat) and it is practically devoid of power to produce direct chemical changes in the human body.
The unit-ampere-refers to the amount or volume of a form of wave-movement in that peculiar condition of matter called ether. .Voltage refers to the force which sets up and keeps up this wave-movement.
The term ohms refers to the amount of resistance or opposition offered to this particular wave-movement.The direct current is, technically speaking, a current of high amperage, i. e., large quantity and low voltage, i. e., it comes with little force. In the indirect current these conditions are reversed, and we have therefore a current of low amperage and high voltage. Indeed here the amount of electricity is only the fractional part of an ampere, but, this small quantity comes with a pressure of hundreds of thousands of volts. The high-frequency, high-voltage currents originate in the indirect or alternating form of electricity. With comparatively simple apparatus we are now able to transform this alternating current so that the alternations occur many thousand times per second, and also there may be obtained an enormous voltage and amperage.
The high-frequency currents, then, are currents of high amperage and also high voltage, however, there is no danger in their use, because, they are not continuous, but alternate, or go back and forth in rapid succession. In the latest form of apparatus as many as 200,000,000 or more alternations occur per second. With the continuous or galvanic current it is possible to kill a human being with 3-10 of an ampere coming at a pressure of about 500 volts; while with the high-frequency currents we may give several amperes at a pressure of between 500,000 and 100,000,000 volts, without the least danger to the person.
Tesla, as far back as the year 1890, proved the comparative lack of danger in using these currents, by allowing them to be passed through his body, when ten ordinary 16 C. P. incandescent lamps held in his hands became fully illuminated. We know it is necessary to have 1/2 ampere for each lamp to get its full luminescence, therefore Tesla’s body must have conducted at least 5 amperes in the experiment cited.” *Bet this is why all the older kree and hoffman galvanic multineeedles only go to 5 !https://books.google.com/books?id=gotXAAAAMAAJ&pg=PA432&focus=viewport&output=text#c_top
6- Rohrer’s Illustrated Book on Modern Baeuty Culture; 1924, Joseph rohrer
“..an abnormal growth of hair is the cause of the most discomfort of all skin defects…the removal of hair has stood the test of not less than 50 yrs {making it 1874}…the kree allows 350 hairs removed per hr as opposed to 50 hairs per hr of single needle, the machines were made as portable and cabnit style.
https://www.amazon.com/Rohrers-illustrated-scientific-modern-culture/dp/B00088FG8K
“In 1924, Dr. Henry Bordier [1863-1942] of Lyon, France suggested using short-wave diathermy…High frequency machines were used to warm parts of the body in ‘medical diathermy’ treatments but they could also generate the high temperatures used in ‘surgical diathermy’ – to excise warts, carbuncles, malignant growths, tonsils and other things – by electrodessication (cautery) or by electrocoagulation….Helena Rubinstein, for example, had at least one machine operating in her London salon in 1929…During the 1930s, despite some controversy over which were better, vacuum tubes began to replace spark-gaps and manufacturers began to produce and sell these new vacuum-tube, high frequency machines to electrologists…When transistors replaced vacuum tubes, timing devices were developed that could produce extremely short bursts of electrical current; much shorter than was possible manually. This resulted in the introduction of what has come to be called the ‘Flash Method’ which used bursts of high-intensity current for a fraction of a second. ..Short-wave, high frequency waves are in the same part of the electromagnetic spectrum as radio waves and can interfere with them. This was aptly demonstrated during the Second World War when British medical diathermy units were deployed for a time in the ‘Battle of the Beams’ to try and block the radio signals the Germans were using…![20210417_224021[1]](https://kittysbelle.files.wordpress.com/2015/10/20210417_2240211.jpg) Beginning in 1930, Hinkel began experimenting with combining direct and alternating currents in the one device... Henri St. Pierre in 1945 and granted in 1948 (U.S. patent No. 2,444,173)…Even though a machine had been built, it took many years of trial and error before St. Pierre developed a working method for removing hair with a combined current, and Arthur Hinkel rightly considers Henri the inventor of the Blend Method. In 1947, Hinkel became a licensed electrologist and together with St. Pierre they set up the St. Pierre Epilator Company in California in 1949. Hinkel also established the A. R. Hinkel Company in 1948.”
Beginning in 1930, Hinkel began experimenting with combining direct and alternating currents in the one device... Henri St. Pierre in 1945 and granted in 1948 (U.S. patent No. 2,444,173)…Even though a machine had been built, it took many years of trial and error before St. Pierre developed a working method for removing hair with a combined current, and Arthur Hinkel rightly considers Henri the inventor of the Blend Method. In 1947, Hinkel became a licensed electrologist and together with St. Pierre they set up the St. Pierre Epilator Company in California in 1949. Hinkel also established the A. R. Hinkel Company in 1948.”
https://www.cosmeticsandskin.com/ded/thermolysis.php
“In 1949, Baer went to work as chief engineer for a small electro-medical equipment firm, Wappler, Inc ., where he designed and built surgical cutting machines, epilators, and low frequency pulse generating muscle-toning equipment.
https://eng.ichacha.net/zaoju/epilator.html
“The first blend was 1946, Hinkle. the first usable and timed thermolysis machine was also 1946…After the name change [Mahler-Instantron] in 1946, the machine above was in a black cabinet the same size, but more boxy looking. Before then all of our machines, professional and home machines, we’re straight galvanic, mostly with batteries…That [small black epilator] is the first automatic time to machine that I speak of that was the predecessor to the machine that you showed. It is thermolysis only.“-Skip Mahler
Electrolysis, Thermolysis and the Blend: the Principles and Practice of Permanent Hair Removal- Arthur Hinkle, professional electrical engineer, 1968
https://archive.org/details/electrolysisther00hink/page/n11/mode/2up
the first “blend” was derived at a time that all the available currents (Galvanic, Ferradic, Sinusodal, etc) were being experimentally combined.
http://www.electrotherapymuseum.com/2007/SeptPaperwork/FischerCombinedGalvanic/index.htm
thermolysis HF output settings
Start with the absolute lowest settings. Be as perfect as possible on insertions. Preferably, use of an insulated probe is best to prevent a HF short. You want the end of the probe in the lower 1/3 of the hair follicle. Start with 1/10 of a second and 1/10 intensity . Insert to the bottom of the follicle and press the peddle being careful to not put outward pressure the needle should be strait into the follicle without twisting the skin.
Gently test the hair with tweezers but discard and move onto another hair if there is any resistance ( there will be, because this setting s too low)
Progressively move on to a new hair and increase the intensity from 1/10 to 2/10 3//10 etc. At the point at which the hair epilates without any traction, smoothly like it’s “lubricated” you have found your working point.
Timing and intensity have a multiplied effect. soif you double the timing, say from 1/10 to 2/10 you need to halve the intensity to provide the same amount of current.
In general, most body hairs will epilate somewhere between 5/10 intensity for 1/10 second to maybe 7/10 intensity. But you slowly increase intensity or timing to find this point . In general i dont recommend increasing timing beyond 1/10 for your first treatments that way you can work with just one factor, intensity.
That, is pretty much how you find your working point . Again however, if you are still learning insertions, please give some galvanic a try before you delve headlong into thermolysis treatments.”
Seana
https://hairtell.com/forum/t/thermolysis-hf-output-and-setting-for-proteus-ep2000/53136/5
how to perform galvanic electrolysis,
electrolysis research corporation, fond du lac, wisconsin
educational video no. 1039A, prod. 3/90, 1990
james e shuster HD
https://www.youtube.com/watch?v=0A0f0TYWIiU&list=LL&index=10
currently hunting down the full video in a library somewhere as its 59 mins, the youtubes only 15mins; meaning the full lecture(or series)also covers blend and thermolysis =^.^=
“prestige was owned by jims sister up untile a few yrs ago, i have the VHS set, they may still have the material.”-mike bono from hairtell forums whose obviously not coming off them.
theres also a dvd set, imagine they were the best from the VHS, so not complete.
– Complications, Side Effects and Tissue Injury in Electrolysis
– Thermolysis
– Blend Electrolysis
– Galvanic Electrolysis
– Guidelines ’97-‘98
https://hairtell.com/forum/t/james-e-schusters-educational-materials/41341
prestige’s old site had..
Complications, Side Effects & Tissue Injury In Electrolysis
Continuing Education Credit
Galvanic Electrolysis Video
How to Make Perfect Insertions Video
Positioning for Needle Electroepilation Video by Kay Lasker
Thermolysis Video
https://hairtell.com/forum/t/what-is-causing-little-red-pinprick-marks/34537/13![20210422_202312[1]](https://kittysbelle.files.wordpress.com/2015/10/20210422_2023121.jpg) prestige now has a 4 dvd set; side effect, thermolysis, blend, galvanic
prestige now has a 4 dvd set; side effect, thermolysis, blend, galvanic
https://www.prestige-supply.com/product/continuing-education-dvds/?attribute_dvd=Complications
*thermolysis, 1989, on dvd, at Victoria University in melbourne australia.
https://www.worldcat.org/title/thermolysis-high-frequency-electrolysis/oclc/225499923
^ galvanic, 1990, same place
https://www.worldcat.org/title/galvanic-electrolysis/oclc/225499915
^ blend, 1993, ”
https://www.worldcat.org/title/blend-electrolysis/oclc/225499898
*also Dr. James Shuster still lives and works!
fond du lac regional clinic, dermatology, Agnesian Healthcare, 920-923-7400
and, St.Agnes hospital, 145 N Main St., Fond Du Lac WI.
awesome vid by Reyuva- galvanic, thermolysis and blend- in solution (modern egg yoke experiment) to show you what happens on the probe to destroy your follicles ability to grow hair.The Galvanic technique is the best for the hair electrolysis for permanent results. It has 90 to 100 % success rate. And is also smooth on the skin. The disadvantage is that it is time consuming, requiring upto 20 to 30 seconds on single hair. We prefer Galvanic technique, it is best for Indian skin since no heat is involved there is no chance of hyper-pigmentation (dark spots). Specially on face and neck we only do galvanic technique.”
https://www.youtube.com/watch?v=srTGm1hu7x4&t=245s
Galvanic lye is a chemically unstable compound which provides free radicals to breakdown tissue and allow separation of the follicle wall surrounding the hair. The follicle containing the hair is comprised of some 6 known layers. Galvanic lye (sodium hydroxide) causes a breakdown of the weaker layers and allows the inner-most part of the follicle to be removed. However, the lye continues to work for some time after the hair is removed, facilitating the death of the outer layers and re-growth cells. Properly applied, galvanic electrolysis will not damage surrounding tissue excessively, nor will it damage the sebaceous glands as galvanic lye encounters difficulty in breaking down the sebum contained in the sebaceous glands.
http://www.electrolysis.net.in/home/index.php/reyuva-electrolysis/galvanic-electrolysis-technique
[note Mrs James speaks of using a toy pen thatd be almost impossible to keep wet, “untile the galvanic foams out the pore”, if you really did that your in for a world of hurt because that means you packed that follicle with lye and its going to keep burning for like an hr,lol. think she’s teasing me.]
 based off my research in 2014 in preparation for the Affordable Care Act, (with indirect help from one Mike Bono who had wrote the original templet for letters pulled from the archives of HairTell) my healthcare team at University of Cincinnati (UC) spent 2015 writing and accumulating letters of medical necessity; of which we have one from my primary care Dr. Sarah Pickle, dermatologist Dr. Kerrith Spicknall, psychiatrist Dr. Shanna Stryker, therapist Evelyn Heffliner. First of the yr in 2016 the affordable care act guidance went into play meaning contractually all Medicaid programs must remove exclusions against gender incongruent care. What is deemed as “trans protections” by the far right are in actuality protections against gender bias in coverage, think mammography in men who get breast cancer too, or a cis woman on testosterone treatments for adrenal gland issues, but until now were denied or deflected thru a lengthy appeall process. In 2016 we had 50 hrs of electrolysis for face and genital “no prior auth required” under Ohio Medicaid, that’s never happened before for anyone. Nor yet, as 4yrs into this and we cant find an electrologist to become an “out of network provider” partly due to refusal of the state to give them billable medical codes. Caresource was trying to dodge it, “sure well cover it good luck turning on an industry that’s historically been considered aesthetic and not setup to bill us, HAHAHA.” left to beg to be reimbursed for out of pocket costs. Instead of playing their game, and after declining Bonos offer to do my work in 2018 because it wouldnt of been repeatable process and he originally intentionally misgendered me (tbh i didnt realize i was using his words against him, thats why he was willing.) later that year i would address Medicaid-oversight and prove discrimination from Caresource to the States Medicaid Oversight; allowing me to switch Medicaid providers before we’re allowed, winning everyone laser coverage, as its unaffected by the 93 OAC amendment directed specifically at electrology. On TDoR 2019, through Cleveland Clinic (CC) and insured via United Health, we had 99+hrs approved, additions to the health team now included a surgeon Dr.Unger and her awesome scheduler Christina Reed, along with 2 laser techs (Lana King UC/ Jaimie Duda CC) currently making the first passes on clients under Medicaid (temporarily interrupted by a covid19 pandemic) but still searching for a new breed of electrologist.
based off my research in 2014 in preparation for the Affordable Care Act, (with indirect help from one Mike Bono who had wrote the original templet for letters pulled from the archives of HairTell) my healthcare team at University of Cincinnati (UC) spent 2015 writing and accumulating letters of medical necessity; of which we have one from my primary care Dr. Sarah Pickle, dermatologist Dr. Kerrith Spicknall, psychiatrist Dr. Shanna Stryker, therapist Evelyn Heffliner. First of the yr in 2016 the affordable care act guidance went into play meaning contractually all Medicaid programs must remove exclusions against gender incongruent care. What is deemed as “trans protections” by the far right are in actuality protections against gender bias in coverage, think mammography in men who get breast cancer too, or a cis woman on testosterone treatments for adrenal gland issues, but until now were denied or deflected thru a lengthy appeall process. In 2016 we had 50 hrs of electrolysis for face and genital “no prior auth required” under Ohio Medicaid, that’s never happened before for anyone. Nor yet, as 4yrs into this and we cant find an electrologist to become an “out of network provider” partly due to refusal of the state to give them billable medical codes. Caresource was trying to dodge it, “sure well cover it good luck turning on an industry that’s historically been considered aesthetic and not setup to bill us, HAHAHA.” left to beg to be reimbursed for out of pocket costs. Instead of playing their game, and after declining Bonos offer to do my work in 2018 because it wouldnt of been repeatable process and he originally intentionally misgendered me (tbh i didnt realize i was using his words against him, thats why he was willing.) later that year i would address Medicaid-oversight and prove discrimination from Caresource to the States Medicaid Oversight; allowing me to switch Medicaid providers before we’re allowed, winning everyone laser coverage, as its unaffected by the 93 OAC amendment directed specifically at electrology. On TDoR 2019, through Cleveland Clinic (CC) and insured via United Health, we had 99+hrs approved, additions to the health team now included a surgeon Dr.Unger and her awesome scheduler Christina Reed, along with 2 laser techs (Lana King UC/ Jaimie Duda CC) currently making the first passes on clients under Medicaid (temporarily interrupted by a covid19 pandemic) but still searching for a new breed of electrologist.
2021 the process is being repeated!
in Cincinnati fake trans orgs are erasing me from my own work by helping Equates to devide and thus gathering my team; Equates protects the Cosmetic Therapy Association who created the barriers i face to finding care or become the missing component. At this time i count my old Sych and Primary care partakers of the coolaid godfunding. im now left to rebuild after burning bridges while standing on them. Dr stryker who had took me off my anxiety meds same time she came back just to be included in the letter building process which denied me casemanagement services yet still ended up verifying discrimiantion from Cinci Job and Family Services; and is now using my freind to make it “consensual”.
![20210531_104908[1]](https://kittysbelle.files.wordpress.com/2015/10/20210531_1049081.jpg)
Dr Pickle whose been working with Stryker and my enemys completely one sided as im left in the dark, is so concerned with recognition even though we havent done this yet, that she lied about having2 black clients, leaving me to figure out how to help them from a patient perspective; so i turned planned parenthood on to the fact id been fighting for my cysters[sic] an that weve had this covered for 5 yrs, and neither UC nor OSU can fire a laser on a black person– in attempt to force them to update their laser for a black patient of theirs, which will cost me my own route to laser thru UC- all because they thought it easier to erase me for someone better benefitting from the existing diode laser. Whole time ive been telln em to update it as i know it wasnt originally bought for hair removal. Thats what happens when you leave major components in the dark, they turn on. Later on Dr Pickle would key me in that i was being trolled by them online pretending to be “admirers”, admitting to lieng about the black patients (that only show up when their dead?) ,and her insitance on working with those who have created my PTSD in the Ohio trans “community”; Which is why Styker took me off my anxiety meds during that terf corruption at Central Clinic, and why Pickle refused to recognize the Cyclical Vomiting Syndrom diagnosis which subsequantly came after, shes just been watching me dissolve. Too her credit she did try to take into context the harm their doing to my own mental and physical healthcare, out of selfish business practices that she herself eventually succumbed to. won’t be gaslighted by my own Dr whose been talking out the corner of her mouth as i hear the excuses from Heartless being repeated. BTW sarah pickle is the “video game museum” and she would rather collect games for her fucking daughter as a way to divest money than help me become licenced to help my people, thats when i realized shes a TERF, just like Sryker ive just been being throttled. remeber the definition of a TERF is :”one who intentional holds or seeks positions of power above trans people with intent to harm or otherwise deny us services”-the whole time at UC i felt like a TERF could read my UC mychart an i was right, it was my own fucking dr.
https://www.uchealth.com/physician/sarah-pickle/
http://www.vgmuseum.com/
in Columbus trans orgs centered around Equates’ funding, who have semi partnered with Vickey- in reality to save face, to the fact its been covered under Medicaid for 5 yrs and the same organization refuses to work with it telling us to “do it ourselves” in context to preop… proven apparently, as im holding the keys to trans healthcare while also being a one-time-cost of schooling an then wed have the tool we all need; point is things are changing and its forcing people to do things- any movement from zero is positive. the schools themselves are addressing curriculum and tuition. laser is now covered, people are slowly starting to get their healthcare.
5/15/21- vickey mickey is using all the funding shes made to recreate the barriers she created 30 yrs ago centered around laser. making the “cosmetic light therapy association of ohio” out of the now non existent “cosmetic therapy association of ohio”. itll be thrown in under the spending bill, which now containes anti lgbt language and wont pass as is; though might, even then its illegall and bravado from the republican party after sending them all back to the barter table over the “fairness” act that woulda extended SERB into the private sector.
In Cleveland there was only one laser tech willing to work on a trans person and Jaimie is on maternity leave 🙂 so that 2019 auth lapsed, because Cleves’ has my Alexandrite wave (ash brown hair coloring). Valerie Katz, the closest we’ve come to an electrologist found the system “too convoluted” to navigate on her own; noone in Cinci was willing to do electrolysis; Amy Day seriously considered it; Kay hit me with a laser that was out of count turning a phase bright blonde; and wouldn’t let Cheri do it unless out of pocket; Jo was concerned with taxes and suggested anouther trans student of hers she couldnt give a name to out of HIPPA that ive yet to find. In general noones going to take the paycut to work with medicaid, at some point I realized I was gonna have to be the one to do it for another.
In all honesty I’m de-platformed by corporate Trans Inc. who run everything deciding who to help and who to kill as they strongarm selling out the narrative; these board members see it as a waste of funding they could use for priveleged pet projects, also these are all poor people issues an therefor inherantly of no concern. Its quite embarrassing to have a kid with no formal training under poverty accomplishing more than they do with all the funding in the world. funding ill never see or be able to access as a disability ridden transwoman in need of services, nor will i be able to be reimbursed thru them if i can become the one providing services under medicaid at an already severely reduced rate.
Litterally doing all the right things, for all the right reasons, going so far as to sacrifice my own healthcare for the greater good, an all i keep hearing ring in my ears is that phrase, “no good deed goes unpunished…” Gears are moving now though in the larger machine; since this work has started I’ve been called a “sociopath” by psychopaths’ covering their ass-ettes, or a “Harbinger” by the raise-o’ the-eyebrow bystander lawyer, and the worst of all “the trans Robinhood” by someone who this work helps one day directly or indirectly.
Medical and Technical Issues in Office Electrolysis and thermolysis; Richard F Wagner Jr MD
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1524-4725.1993.tb00391.x
The Medicare Transitional Pass-Through Payment (TPT) program is designed to foster innovation and increase access to cutting-edge treatments that benefit patients. The Centers for Medicare and Medicaid Services (CMS) believes the program is important for hospitals to receive TPT payment for products that offer substantial clinical improvement. One goal of the program is to target TPT payments for those devices where cost considerations might be most likely to interfere with Medicare patient access.
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Downloads/catapp.pdf
419.66
eligibility-
(2) The device is determined to be reasonable and necessary for the diagnosis or treatment of an illness or injury or to improve the functioning of a malformed body part (as required by section 1862(a)(1)(A) of the Act).
criteria for device categories-
(2) CMS determines either of the following: (i) The device to be included in the category has demonstrated that it will substantially improve the diagnosis or treatment of an illness or injury or improve the functioning of a malformed body part compared to the benefits of a device or devices in a previously established category or other available treatment; or (ii) For devices for which pass-through payment status will begin on or after January 1, 2020, as an alternative pathway to paragraph (c)(2)(i) of this section, the device has received FDA marketing authorization and is part of the FDA’s Breakthrough Devices Program.
(d) Cost criteria. CMS considers the average cost of a category of devices to be not insignificant if it meets the following conditions:
(1) The estimated average reasonable cost of devices in the category exceeds 25 percent of the applicable APC payment amount for the service related to the category of devices.
(2) The estimated average reasonable cost of the devices in the category exceeds the cost of the device-related portion of the APC payment amount for the related service by at least 25 percent.
(3) The difference between the estimated average reasonable cost of the devices in the category and the portion of the APC payment amount for the device exceeds 10 percent of the APC amount for the related service.
(h) Amount of pass-through payment. Subject to any reduction determined under 419.62(b), the pass-through payment for a device is the hospital’s charge for the device, adjusted to the actual cost for the device, minus the amount included in the APC payment amount for the device.
https://www.law.cornell.edu/cfr/text/42/419.66
Looking at a case study hospital–a large urban teaching center–results show that the modified pass-through approach is the most advantageous, providing the largest cash flow.
https://pubmed.ncbi.nlm.nih.gov/10300594/
Medical Necessity Statements
AAP American Academy of Pediatrics, a letter from their president
http://www.aappublications.org/news/2016/08/03/Letter072816
AAFP American College of Family Physicians, In 2007, an AAFP Commission declared that the association has a policy opposing any form of patient discrimination and stated its opposition to the exclusion of transgender health care: “RESOLVED, That the American Academy of Family Physicians endorse payment by third party payors to provide transsexual care benefits for transgender patients.”
http://www.aafp.org/dam/AAFP/documents/about_us/special_constituencies/2012RCAR_Advocacy.pdf
ACOG American College of Obstetricians and Gynecologists
“Transgender individuals face harassment, discrimination, and rejection within our society. Lack of awareness, knowledge, and sensitivity in health care communities eventually leads to inadequate access to, underutilization of, and disparities within the health care system for this population. Although the care for these patients is often managed by a specialty team, obstetrician-gynecologists should be prepared to assist of refer transgender individuals with routine treatment and screening as well as hormonal and surgical therapies. The American College of Obstetricians and Gynecologists opposes discrimination on the basis of gender identity and urges public and private health insurance plans to cover the treatment of gender identity disorder.”
http://www.acog.org/Resources_And_Publications/Committee_Opinions/Committee_on_Health_Care_for_Underserved_Women/Health_Care_for_Transgender_Individuals
ACP American College of Physicians, calls for clinical LGBT competency recognizing disparency of care
http://annals.org/article.aspx?articleid=2292051
AMA American Medical Association
http://www.imatyfa.org/wp-content/uploads/2013/06/ama_resolution_122.pdf
“An established body of medical research demonstrates the effectiveness and medical necessity of mental health care, hormone therapy and sex reassignment surgery as forms of therapeutic treatment for many people diagnosed with GID … Therefore, be it RESOLVED, that the AMA supports public and private health insurance coverage for treatment of gender identity disorder.”
http://www.tgender.net/taw/ama_resolutions.pdf
AMSA American Medical Student Association,issues guidance for care of transgender patients
http://www.amsa.org/advocacy/action-committees/gender-sexuality/transgender-health/
APA American Psychology Association
As stated in the Policy on Transgender, Gender Identity & Gender Expression Non-Discrimination, the APA “opposes all public and private discrimination on the basis of actual or perceived gender identity and expression and urges the repeal of discriminatory laws and policies” and “calls upon psychologists in their professional roles to provide appropriate, nondiscriminatory treatment to transgender and gender variant individuals and encourages psychologists to take a leadership role in working against discrimination towards transgender and gender variant individuals[.]”
The “APA recognizes the efficacy, benefit and medical necessity of gender transition treatments for appropriately evaluated individuals and calls upon public and private insurers to cover these medically necessary treatments.”
http://www.apa.org/news/press/releases/2008/08/gender-variant.aspx
APA guidelines
http://www.apa.org/practice/guidelines/transgender.pdf
AAFP American Academy of Family Physicians (resolutions 1002-1006)
http://www.aafp.org/dam/AAFP/documents/about_us/special_constituencies/2012RCAR_Advocacy.pdf
APHA American Public Health Association,The APHA issued a policy statement concluding that, “transgendered individuals are not receiving adequate health care, information, or inclusion within research studies because of discrimination by and/or lack of training of health care providers and researchers; herefore…”The APHA thus “Urges researchers and health care workers to be sensitive to the lives of transgendered individuals and treat them with dignity and respect, and not to force them to fit within rigid gender norms. This includes referring to them as the gender with which they identify; Urges researchers, health care workers, the National Institutes of Health, and the Centers for Disease Control and Prevention to be aware of the distinct health care needs of transgender individuals; and Urges the National Institutes of Health and the Centers for Disease Control and Prevention to make available resources, including funding for research, that will enable a better understanding of the health risks of transgendered individuals, especially the barriers they experience within health care settings…”
http://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2014/07/29/09/18/the-need-for-acknowledging-transgendered-individuals-within-research-and-clinical-practice
DoD Dept of defense, effective oct 1st 2016
- Service members with a diagnosis from a military medical provider indicating that gender transition is medically necessary, will be provided medical care and treatment for the diagnosed medical condition. Recommendations of a military medical provider will address the severity of the Service member’s medical condition and the urgency of any proposed medical treatment. Medical advice to commanders will be provided in a manner consistent with processes used for other medical conditions that may limit the Service member’s performance of official duties.
http://www.defense.gov/Portals/1/features/2016/0616_policy/DoD-Instruction-1300.28.pdf
HHS U.S. Department of Health and Human Services, released guidelines 5/14/16
“The final rule helps consumers who are seeking to understand their rights and clarifies the responsibilities of health care providers and insurers that receive federal funds. The final rule also addresses the responsibilities of issuers that offer plans in the Health Insurance Marketplaces. Among other things, the final rule prohibits marketing practices or benefit designs that discriminate on the basis of race, color, national origin, sex, age, or disability. The final rule also prohibits discriminatory practices by health care providers, such as hospitals that accept Medicare or doctors who participate in the Medicaid program.”
http://www.hhs.gov/about/news/2016/05/13/hhs-finalizes-rule-to-improve-health-equity-under-affordable-care-act.html
NASW National Association of Social Workers-“NASW supports the rights of all individuals to receive health insurance and other health coverage without discrimination on the basis of gender identity, and specifically without exclusion of services related to transgender or transsexual transition…in order to receive medical and mental health services through their primary care physician and the appropriate referrals to medical specialists, which may include hormone replacement therapy, surgical interventions, prosthetic devices, and other medical procedures.”
https://www.socialworkers.org/da/da2008/finalvoting/documents/Transgender%202nd%20round%20-%20Clean.pdf
NCCH National Commission on Correctional Healthcare
“The health risks of overlooking the particular needs of transgender inmates are so severe that acknowledgment of the problem and policies that assure appropriate and responsible provision of health care are needed…Because prisons, jails, and juvenile justice facilities have a responsibility to ensure the physical and mental health and well-being of transgender people in their custody, correctional health staff should manage these inmates in a manner that respects the biomedical and psychological aspects of a gender identity disorder (GID) diagnosis.”
http://www.ncchc.org/filebin/Positions/Transgender-Transsexual-and-Gender-Nonconforming-Health-Care.pdf
PA Phycological Association of Ohio’s statement on ending conversion therapy
http://www.ohpsych.org/about/2016/02/13/ending-conversion-therapy-statement/
WPATH- World Professional Association on Transgender Health, “Medically necessary sex reassignment procedures also include complete hysterectomy, bilateral mastectomy, chest reconstruction or augmentation as appropriate to each patient (including breast prostheses if necessary), genital reconstruction (by various techniques which must be appropriate to each patient, including, for example, skin flap hair removal, penile and testicular prostheses, as necessary), facial hair removal, and certain facial plastic reconstruction as appropriate to the patient.”
http://www.wpath.org/site_page.cfm?pk_association_webpage_menu=1352&pk_association_webpage=3947
WPATH reverification of necessity
https://s3.amazonaws.com/amo_hub_content/Association140/files/Letter%20Re_Medical%20Necessity%20of%20Electrolysis_7-15-15.pdf
http://www.wpath.org/site_page.cfm
WMA World Medical Association
http://www.wma.net/en/40news/20archives/2015/2015_36/index.html
WHO world health organisation, document explaining social inequality concerning access to health care and the detriment to health
http://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf
a joint letter from the APA, APSPA, NASW, and AAPCSW
“The nation’s leading mental health professional organizations are expressing dismay over the spate of recent bills and laws that would allow for individuals and businesses to deny services, employment and housing to LGBT people under the guise of religious freedom. Studies confirm that discrimination, bias and prejudice have negative consequences on one’s mental health and overall well-being. Specifically, research has linked anti-LGBT discrimination to increased risk of depression, anxiety and substance use. And studies show that lesbian, gay and bisexual youth are up to six times more likely to attempt suicide while 41 percent of transgender people report having made a suicide attempt.
It is important to note that several studies also show marked increases in overall physical and mental health when governments enact laws and policies, such as the executive orders recently signed by Pennsylvania Gov. Tom Wolf that strengthen equality for LGBT people. Community and family acceptance has also been shown to contribute significantly to fewer occurrences of depression, anxiety and suicidality for LGBT youth.
Our organizations have strong ongoing commitments to promote the health and well-being of LGBT adults and youth; to eliminate violence against LGBT people; and to support full equality in areas such as marriage, employment, housing, public accommodation, military service, licensing, parenting, adoptions and access to legal benefits.
We urge states to reject these harmful and discriminatory bills and to repeal such laws that have already passed.”
http://www.apsa.org/sites/default/files/Joint_Statement_Religious_Freedom_Laws_0.pdf
 “A precedent has already been set indicating that depilatory treatments are “medical care” for insurance purposes (Abernathy v. The Prudential Insurance Company of America, No. 21178, Supreme Court of South Carolina, March 31, 1980). In this case Plaintiff brought suit against her insurer after it refused to reimburse her for the cost of depilatory treatments (i.e. electrolysis) which had been recommended by her physician. The policy included as “eligible expense” charges for “doctors’ services for surgical procedures and other medical care”, and contained a provision excluding “anything not ordered by a doctor or not necessary for medical care of illness”. The South Carolina State Supreme Court affirmed a verdict for the plaintiff, noting that there is no requirement that “medical care … be performed by or under the direction of licensed medical personnel”. Further, the court held, since plaintiff underwent treatments pursuant to her physician’s advice, such expenses were medically “necessary and were not excluded from coverage under the policy”. Again, if your health care provider has covered any part of your treatment that has anything to do with why your hair removal is needed, you have a good chance to beat the money out of them in small claims court.”
“A precedent has already been set indicating that depilatory treatments are “medical care” for insurance purposes (Abernathy v. The Prudential Insurance Company of America, No. 21178, Supreme Court of South Carolina, March 31, 1980). In this case Plaintiff brought suit against her insurer after it refused to reimburse her for the cost of depilatory treatments (i.e. electrolysis) which had been recommended by her physician. The policy included as “eligible expense” charges for “doctors’ services for surgical procedures and other medical care”, and contained a provision excluding “anything not ordered by a doctor or not necessary for medical care of illness”. The South Carolina State Supreme Court affirmed a verdict for the plaintiff, noting that there is no requirement that “medical care … be performed by or under the direction of licensed medical personnel”. Further, the court held, since plaintiff underwent treatments pursuant to her physician’s advice, such expenses were medically “necessary and were not excluded from coverage under the policy”. Again, if your health care provider has covered any part of your treatment that has anything to do with why your hair removal is needed, you have a good chance to beat the money out of them in small claims court.”
http://www.hairtell.com/forum/ubbthreads.php/topics/1410/6.html
transcend legal has 2 pages of various insurance policy across states that recognize coverage of electrolysis as medically necessary
https://transcendlegal.org/health-insurance-medical-policies/permanent-hair-removal
SFHP will cover electrolysis and laser hair removal for the following surgeries
- Vaginoplasty (genital area and face)
- Metoidioplasty (exclusively to the genital area)
- Phalloplasty (genital area and graft site)
https://www.sfdph.org/dph/files/THS2/SFHP-MedicalCriteriaTransgenderCare-020215.pdf
^ As of February 20, 2015 San Francisco Health Plan amended their guidelines to include limited coverage for facial hair removal for transgender patients who meet medical necessity. SFHP thus far has indicated that they will only approve facial hair removal for patients who also have a Prior Authorization approved for vaginoplasty. While it is clear that the medical necessity for facial hair removal should be considered separately from surgical status and that these procedures should be authorized independently, SFHP is currently not interpreting coverage this way. Expanded coverage for medically necessary gender-related procedures has often been gained through winning coverage for individual patient cases. This is typically a lengthy process that requires a series of denials and strong provider advocacy documenting medical necessity. For patients who have an approval for vaginoplasty with SFHP, facial hair removal is more likely to be approved, however SFHP could still deny requests on a case by case basis. This guide provides an overview of how to make a referral for facial hair removal, how to fill out Prior Authorization forms, what clinical documents to attach to them, and how to appeal a denial.
https://www.sfdph.org/dph/files/THS2/SFHP-FacialHairRemovalProviderGuide-071715.pdf
NY state covers electrolysis as preoperative for vaginoplasty and metoplasty
https://www.health.ny.gov/health_care/medicaid/program/update/2015/2015-06.htm
Health and Human Services, “By including gender identity in the regulations, they said, insurance and service providers would have to cover drugs, surgeries, and other services associated with some transgender people’s gender transitions.”
https://www.buzzfeed.com/dominicholden/new-obamacare-rule-protects-transgender-patients?utm_term=.huR7NDbvn#.tlOx0nMy5
^HHS, final ruling
https://s3.amazonaws.com/public-inspection.federalregister.gov/2016-11458.pdf
Herman cost benefits of trans health benefits; Costs and Benefits of Providing Transition-Related Health Care Coverage in Employee Health Benefits Plans FINDINGS FROM A SURVEY OF EMPLOYERS
http://williamsinstitute.law.ucla.edu/wp-content/uploads/Herman-Cost-Benefit-of-Trans-Health-Benefits-Sept-2013.pdf
Hopkins social implications for coverage of transgender people
http://www.jhsph.edu/news/news-releases/2015/study-paying-for-transgender-health-care-cost-effective.html
June 17, 2021, the US Supreme Court upheld the Affordable Care Act Thursday in a 7-to-2 vote, rejecting claims by the challengers.This marks the third time the Supreme Court spared the Obama-era law from GOP attacks. The mandate was also upheld in 2012 5 to 4.
https://www.medscape.com/viewarticle/953297
consider pain prescription for Tylenol 3 and EMLA cream for mine. though any reimbursement counts, your spironolactone (that your prolly’ already on) is also being used to combat hirsutism.
https://youngwomenshealth.org/2014/02/25/spironolactone/
Emla topical cream is 2.5% lidocaine/2.5%prilocaine, this is typically the only pain creame covered by insurance because its entire process from creation to implementation is well studied an approved by the FDA. the patents of the compound pharmacys while using the same ingrediants- long term and comparative studys are non existent so its considered liscenced safe for production and sale by the FDA, but is considered experimental not the “standard medical prescription” so does not yet meet criteria for coverage by insurance.
https://www.webmd.com/drugs/2/drug-2358-8170/emla-topical/lidocaine-prilocaine-cream-topical/details
“NumbSkin Plus is 10.56% pure Lidocaine, and NumbSkin Foaming Soap is 4% Lidocaine, which works well together to give maximum numbness to reduce pain when applied properly. it is the strongest OTC topical numbing agent you can purchase without a prescription.”-Diane Rolling
https://professionalelectrolysisservices.com/how-can-you-make-your-pain-feel-better/
Custom Scripts Pharmacy makes a 20% lidocaine/prilocaine mixture with .25% phenylephrine (same strength as preparation H). you must have a physician write you a script for this, they wont even talk to you, only your dr- but once they have its a quick shipment to your house, your directly billed and you can reorder as many that were prescribed.
https://www.csrx.us/contact-us/
http://idnps.com/basics/ultrasound-study/5-2-sonophoresis/
pg 128, depilatories, creams and paste for hair removal, dicks encyclopedia of practical receipts and processes, or how they did it in the 1870’s
https://archive.org/details/encyclopediaofpr00dickrich
![20201225_143813[1]](https://kittysbelle.files.wordpress.com/2015/10/20201225_1438131.jpg) ^1n the early 1930s mass production took over the creation of depilatories. before then each family had its own recipe, catered and refined to its specific body type. These depilatories worked better than what is in market today because it is marketing to a wide body range while ensuring its product doesn’t burn one of them. If your grandma did a geneology, ask her if anyone had a recipe for a family depilatory cream in the 1800s and use it.
^1n the early 1930s mass production took over the creation of depilatories. before then each family had its own recipe, catered and refined to its specific body type. These depilatories worked better than what is in market today because it is marketing to a wide body range while ensuring its product doesn’t burn one of them. If your grandma did a geneology, ask her if anyone had a recipe for a family depilatory cream in the 1800s and use it.
it is these same industries that suppress the populous’ ability to access medical treatment for hair issues, or research into relatively simply gene suppression to shut down the signals that cause hair to even grow. it is to their financial benefit to constrain access and therefor charge more not only for current products like razors, and treatment like electrolysis or laser, but future technologies derived of scientific research that would make these aggravations unneeded. *define classism
https://books.google.com/books/about/Plucked.html?id=LZvsCwAAQBAJ
A technique for genetic modification of hair follicles was developed which results in efficient alteration of the hair shaft phenotype. High-level in vivo transgene expression was maintained in hair follicles such that growing hair shafts were phenotypically altered. Mouse anagen skin fragments, maintained in histoculture, were genetically modified at high efficiency with adenoviral-GFP. The histocultured skin fragments were treated with collagenase which made hair follicles accessible to the adenoviral GFP gene, allowing high-efficiency transduction. These skin fragments were subsequently grafted on to nude mice where GFP was readily visualized in as many as 75% of hair follicles. Most follicles produced GFP-fluorescent growing hair shafts. This technique has produced efficient genetic modification of the hair shaft.
At the onset of each new anagen, stem cells (largely in the “bulge area” of the hair follicle) proliferate and give rise to progenitor matrix cells. In turn, these generate the hair shaft and its surrounding layers. The matrix cells determine the characteristics of the new hair and are, therefore, an attractive target for genetic modification.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC130596/
Vaniqua (which wasnt covered by caresource but maybe your insurance), a cream for reducing the speed of hair growth, 70 bucks for a month supply, wanna try it after readn. this also is a great place to know your not alone with your hair issues even knowing other women get it too somehow helps?
http://www.soulcysters.net/showthread.php/345083-Endocrinologist-Lab-Results-can-a-GP-read-diagnosis-Asymmetrial-Thyroid-ROP?goto=nextnewest
Pain Management
*im currently builing an ecco the dolphin collection (going round the world with it), to build a giant shadow box wall art: consisting of games reviews/ads/etc and a hologram ill have made- as an educational tool youll never forget once you see it in the right medium, and ill use it to explain the importance of hydration when they ask me Q:”whats the deal with the dolphins?”… A:”i want you hydrated like ecco the friggn dolphin, remember how hard that game was an how you had to do stuff in the past to affect the future, well hydrations kinda like that..”
stay hydrated! -“Moisture is needed in the skin to properly conduct both RF and Galvanic current. Dry tissue is greatly unaffected.”-Divide your weight by 2. That’s how many ounces of water you should aim for per day. For example, say a person weighs 150 pounds. 150 divided by 2 is 75. So that person would drink 75 ounces of water a day.” theres a difference between hydration and hydration on clinical day- it takes days, even weeks, to hydrate, so on electro day try not to drink so much ya gotta go during your apointment!
http://permanent-hair-removal-info.com/electrolysis-hair-removal-better-when-wet/
From a Cardiac Specialist
“Drinking water at a certain time maximizes its effectiveness on the body
2 glasses of water after waking up – helps activate internal organs [drink it all, no tossouts!]
1 glass of water 30 minutes before a meal – helps digestion
1 glass of water before taking a bath – helps lower blood pressure
1 glass of water before going to bed – avoids stroke or heart attack, water at bed time will also help prevent night time leg cramps. Your leg muscles are seeking hydration when they cramp and wake you up with a Charlie Horse.”
https://www.cpr-n-more.com/heart-attacks-water/
from an OSU Dentist, Oshin Sharma
“when you eat something the acids in the food are attacking your enamel which weakens it so you shouldn’t brush immediately after meals but wait a half hr for the enamel to restrengthen. in the meantime drinking a glass of water immediatly after a meal or any food helps by diluting those acids assisting your saliva with time to neutralize those acids, without causing any harm”
protip- since were talking about dental habits, when flossing you can feel the hardened tarter as a little “clink” that catches with your dental floss pic, thats what your going after.
https://www.mayoclinic.org/healthy-lifestyle/adult-health/expert-answers/brushing-your-teeth/faq-20058193
use those 2sets ^ of most optimal water times, and set alarms on your phone that coincide with your daily habits, your now guaranteed to meet requirements for hydration! Though in reality this is really a multitude of conscious decisions you need to make though-out the day, everyday. Choosing water over other substances; Soda Pop and coffee actually dehydrates you, even if its 98% water its the sugars and caffeine in it that cause you to urinate more often, thus long term loosing more moisture than your retaining from it- but outside cognitive you prolly wont notice how it fully hampers your bodies development until the age of cellular decay.
“The researchers looked at data from 2009-2012 on more than 4,000 children and adolescents aged 6 to 19 years who participated in the National Health and Nutrition Examination Survey, a study of the health of U.S. children and adults conducted each year by the Centers for Disease Control and Prevention. They used urine osmolality—a measure of how concentrated a person’s urine is—to determine whether or not participants were adequately hydrated. They found that a little more than half of all children and adolescents weren’t getting enough hydration. Boys were 76% more likely than girls, and non-Hispanic blacks were 34% more likely than non-Hispanic whites, to be inadequately hydrated. Notably, nearly a quarter of the children and adolescents in the study reported drinking no plain water at all.”
https://www.hsph.harvard.edu/news/press-releases/study-finds-inadequate-hydration-among-u-s-children/
^ so dont worry if it takes a bit of time or effort to get started drinking enough fluids.
“do anything for 21 days and it becomes a habit”
“Researchers from University College London examined the new habits of 96 people over the space of 12 weeks, and found that the average time it takes for a new habit to stick is actually 66 days; furthermore, individual times varied from 18 to a whopping 254 days. The take-away message here is that if you want to develop a new behavior, it will take at least two months, and you shouldn’t despair if three weeks doesn’t do the trick – for most people that’s simply not enough.”
dont give up!
https://www.sciencealert.com/how-long-it-takes-to-break-a-habit-according-to-science
“We have examined brain activity associated with thirst and pain experiences in a single group of subjects, to examine the commonality and differences of activation in the anterior cingulate cortex and insulae. Pain perception was enhanced under conditions of contemporaneous thirst, whereas thirst ratings were unaffected by pain. These sensations elicited activations in adjacent regions of the anterior cingulate cortex, but in different locations in the insulae, suggesting a functional topography for pain and thirst in the two regions. The concurrence of pain and thirst were notable for activations in the pregenual cingulate cortex and ventral orbitofrontal cortex that were not in evidence for either sensation in isolation, pointing toward an integrative role for the regions in the processes of context-dependent changes in sensation.“
https://www.pnas.org/content/103/7/2416.full
” a sympathetic dentist”, usually this means ones own personal dentist whos licensed to numb around the jaw. this link is to an interesting place that uses anesthesiology in Cincinnati..(look further into)
https://nofeardentist.com/your-first-visit/paymentinsurance/
anesthesiologists are also for hire, theres one that will come to a controlled professional environment an keep you numb for 8 hrs to the cost of 4k.
twilight
how controlled breathing helps regulate blood pressure, taps into the emotion control center, and may boost the immune system
https://www.forbes.com/sites/daviddisalvo/2017/11/29/how-breathing-calms-your-brain-and-other-science-based-benefits-of-controlled-breathing/
i find myself doing this while under an hrs worth of electrolysis..
it would be beneficial for the electrologist to not only be zapping hair but leading a trance.
choreographed with the breathing of the patient, in basic 5-2-5 steps.
1-breath in threw your nose for 5 secs, not 5 breaths just continued 5 secs.
2- hold that breath for 2 secs.
3- release that breath continually for 5 secs.
4- the “chi” that is the finger circle is about your energy, everyone has an electromagnetic field regardless if you believe in spirituality, this is science. when you connect you are redirecting your current to stay within your body instead of leaching out,*this current is not the electrology machines doing, which is on a diffrent level, this is your own interference, or “leakage”. remebr RF machines do interfer with radio waves- the same as your physical proximity to a common radio antenna affects its reception…
5-just like staying hydrated helps the electrology process work, so does having a clear mind. do not be hungry, dont be sleepy, dont be nicn’ for a smoke, dont need to use the bathroom, you need to be content physically and mentally. where your body and mind wants for nothing.
6-focus on those breathes going in an out………exhale..5..4..3..2..1..sometimes a little longer like..6, to exhaust as much carbon monoxied, to have more room for more oxygen on the next rep.
7- if your mind starts to wander to want or worry, simply be aware of it, and bring yourself back to focusing on the air filling your lungs an releasing..5..2..5..
8- by working with a client in trance using mindfullness techniques, being attune with their own breathing, let your galvanic or blend flow in synchrony with their breaths. a total of 12 secs per breath, blend requires 6-18 secs to detach a hair (modest first pass reduction so as not to unnecessarily retreat), so by staying within the time-frame of the breath or between end+beginning breaths, you should be able to insert, treat, and remove a hair, if not dont get ahead, this is a time consuming process, stay with us. if it needs rezapped to let loose, wait until the next breath. 1 hair per breath.
9- now you have a timeline of how much hair you can guarantee within an hr or 15 min intervals. you learn based simply on appearance how much hair per square inch there is based on coarseness and color so you use that to estimate based on the 12 sec breaths, to bid sections of hair removal. allowing you to charge a flat rate for a face or genital area. remember your not there to make money but to help the patient overcome hair issues. therefore you must see the patient as a project to be completed, not perpetual clientele.
this is the basic first step to a progressive treatment plan.
10-other implementations can be added such as background noise like water or fans or white noise or song, as potential distraction. focus on staying with the patients breathing, talk them through, when you notice pain and aggravation.. start counting, leading the patient..1…2…an go through a whole breath without neeedle giving them a chance to refocus, before you treat the follicle again. this saves you time, instead of a patient getting up and walking around or needing a min break you keep the process moving with a 12 sec break here and there as needed per the threshold of the client.
11- this does require patience of the part of the technician, it also requires the patient to do their best to maintain.
12-(you should be near to fully exhaled by now)
https://www.gaiam.com/blogs/discover/meditation-101-techniques-benefits-and-a-beginner-s-how-to
[From; Mike Bono on a Hairtell thread]
LETTERHEAD
MEDICAL CLAIMS DEPARTMENT
XYZ INSURANCE CO.
CLAIMS DEPARTMENT / OR MANAGER
RE: (patient�s name) Policy No. #000000
Dear Ms./Mr……………
I have prescribed for my patient, Ms. ………….., electrolysis
(procedure 17380) as a consequence of a hormonal imbalance resulting in
hirsutism (excessive and abnormal growth of hair in a distribution not
normal in a female… (diagnosis 704.1).
I am writing you to clarify the medical necessity of this treatment.
Hair removal is NOT cosmetic in these patients because
A. a medical condition causes the hair growth.
B. permanent removal of hair is necessary to restore the patient to normal function.
C. the physician can measure the effectiveness of medication by
monitoring the presence or absence of new hair growth in the areas involved only after
electrolysis therapy. Since no two patients respond in a similar manner to a given dose of any medication, dosage MUST be individualized to minimize potential �side effects�. Electrolysis, therefore, is instrumental in establishing the most effective dose of medication, consequently, the electrolysis procedure is diagnostic as well as therapeutic.
D. To achieve maximum benefits for the patient with Hirsutism it
is necessary to include electrolysis of the follicle concomitantly with medical therapy or else the
patient is denied the benefit of the current body of medical knowledge regarding treatment of her condition. Also, it is unethical for a physician to withhold any information from a patient that the physician knows to be effective.
E. Electrolysis is standard, current medical practice and is the
only permanent treatment for hirsutism in this medical condition and has been certified as medically indicated and necessary by a disinterested physician, Dr. …… , a Board Certified Endocrinologist (or Gynecologist).
F. There is industry precedent in Massachusetts and a number of states for coverage of this procedure.
Please contact me if I can be of further assistance
Yours truly
XXXXXXX M.D.
————————————————–
Very important phrases…………
1. A hormonal imbalance resulting in hirsutism (excessive and abnormal
hair growth not normal in a female 2. Is NOT COSMETIC in these
patients. 3. A medical condition causes the hair growth. 4. Permanent
removal is necessary to restore the patient to normal function. 5. the
physician can measure the effectiveness of medication by monitoring the
presence or absence of new hair growth ONLY AFTER electrolysis therapy.
6. no two patients respond in a similar manner to a given dose of any
medication.� 7. dosage MUST be individualized to minimize potential
side effects. 8. Electrolysis, therefore, is instrumental in
establishing the most effective dose of medication. 9. the electrolysis
procedure is diagnostic as well as therapeutic (this is vital because
ALL DIAGNOSTIC TESTS ARE COVERED 100% IN VIRTUALLY ALL POLICIES). 10.
To achieve maximum benefits for the patient it is necessary to include
electrolysis. 11. or else the patient is denied the benefit of the
current body of medical knowledge regarding treatment 12. It is
unethical for the physician to withhold any information from a patient
that the physician knows to be effective. 13. Electrolysis is current
standard medical practice. 14. the only treatment for hirsutism in this
medical condition. 15. has been certified as medically necessary by a
disinterested physician (this means the physician has no vested
interest in electrology other than to see the patient get the most
effective treatment with no financial gain for the physician). 16.
there is industry precedent for coverage for this procedure (in law
they often resort to �precedent� so this VIP). In addition, read the
policy to see if there is any wording that refers to �diagnosable and
treatable disorders� which this is as opposed to a �cosmetic
procedure�. Electrolysis for cosmetic purposes would be limited to
eyebrows, underarms, bikini line, raising the hairline on the forehead.
All other areas could be part of a medical problem.
Do not let them push you around. Their tactics usually involve denying
and delaying all these claims. Send all correspondence by �return
receipt requested mail� so you will have proof the letter was sent and
received. Sometimes they claim they �lost� the letter but if you get no
reply send another with a note there will be more and it is doubtful if
they lose all correspondence. Lastly you can take them to small claims
court after about only $1000 of treatments. Ins companies do not want
to go to court under any circumstance as they know nobody likes them
and the penalties are usually severe. They will try to call your bluff
every time as the know no lawyer will take a case for less than $50,000
so they figure you will drop the whole thing due to frustration.”
http://www.hairtell.com/forum/ubbthreads.php/ubb/showflat/Number/1341/site_id/1
Electrology and the Hirsute Polycystic Ovary Syndrome Patient, remember if it is covered for one gender it must be covered for the other! regardless what you may think you know of trans women.
https://www.aielectrology.com/news_7.shtml
how to code and treat for insurance
http://transhealth.ucsf.edu/trans?page=guidelines-hair-removal
‘L689’ (L68.9) Diagnosis – Hypertrichosis, unspecified, The code is valid for submission on a UB04
http://www.hipaaspace.com/Medical_Billing/Coding/ICD-10/Diagnosis/L689
L68.2 Localized hypertrichosis
is a billable medical code that can be used to specify a diagnosis on a reimbursement claim.
http://www.mdhealthresource.com/icd-10-cm-medical-codes/L68.2
“The use of lasers has become commonplace in the cosmetic cutaneous arena. Dissatisfaction with currently available hair removal techniques has led to enormous interest in laser and light source treatment for hair removal. The principle of selective photothermolysis can be applied to hair much as it is applied to the treatment of a variety of pigmented and vascular lesions of the skin. Temporary hair removal is currently available with a variety of systems. Occasional permanent hair removal has been noted. With a greater understanding of hair biology and continued improvement in technology, the elusive goal of permanent hair removal with minimal risk is likely to be met in the near future.”
https://www.skinandlasers.com/wp-content/uploads/2013/11/hair2.pdf
“This encyclopedia is authored by Dr. Rüdiger Paschotta.” An awesome resource in becoming familiar with the technical aspect behind the guts in whichever laser you decide on from research to medical to industrial, all forms of amplified photonics are covered in an easy to navigate learners guide to advanced theory and practice.
https://www.rp-photonics.com/lasers.html
“Lasers are sources of high-intensity light with the following properties:
Monochromatic — the radiation is of a single wavelength
Coherent — the light beam waves are in phase
Collimated — the light beams travel in parallel
Laser light can be accurately focused into small spots with very high energy. The light is produced within an optical cavity containing a medium, which may be a gas (eg, argon, krypton, carbon dioxide), liquid (eg, dye) or solid (eg, ruby, neodymium:yttrium-aluminium-garnet, alexandrite). The process involves excitation of the molecules of the laser medium, which results in the release of a photon of light as it returns to a stable state. Each medium produces a specific wavelength of light, which may be within the visible spectrum (violet 400 through to red 700nm) or infrared spectrum (more than 700 nm).”
https://dermnetnz.org/topics/lasers-in-dermatology/
first laser was actually a MASER
“A method for amplifying light had its origins in an idea Einstein developed in 1916.
Scientists and engineers pushed radio techniques to ever shorter wavelengths, radio (meters) and radar (centimeters, then millimeters) In the 1930s some hoped they were on the verge of creating a “death ray.” That turned out to be unworkable, but the effort led to something better — radar. By 1940, ingenious devices could generate rays with wavelengths of a centimeter or less.
By 1954 they had the device working. Townes called it a MASER, for “Microwave Amplification by Stimulated Emission of Radiation.”
light rays could be thought of as electro- magnetic waves — similar to radio waves, but with much shorter wavelengths…The only difference between one ray and another is the length of its wave. (We can also say the frequency is different, the frequency being the number of waves that pass a point each second as the ray moves through space.)
in the 1930s scientists could have built a laser. They had the optical techniques and theoretical knowledge — but nothing pushed these together. The push came around 1950 from an unexpected direction. Short-wavelength radio waves, called microwaves, could make a cluster of atoms vibrate in revealing ways (a technique called microwave spectroscopy).
Radar equipment left over from World War II was reworked to provide the radiation.
One day in 1957, Charles Townes, studying the equations for amplifying radiation, he realized that it would be easier to make it happen with very short waves than with far-infrared waves. He could leap across the far-infrared region to the long-familiar techniques for manipulating ordinary light.
Gould and Schawlow found the key — put the atoms you wanted to stimulate in a (optic chamber) long, narrow cavity with mirrors at each end. The rays would shuttle back and forth inside so that there would be more chances for stimulating atoms to radiate. One of the mirrors would be only partly silvered so that some of the rays could leak out.
Maiman realized the source did not have to shine continuously,he found a very bright lamp with a helical shape. Just right, he thought, for fitting a ruby inside. He assembled the components with the aid of an assistant, Irnee d’Haenens, and on May 16, 1960 they observed pulses of red light. It was the world’s first laser.
it would revolution industry; fiberoptic cable, scanners, holograms , printers, etc used to mine cut drill well, and of course perform surgery.
The average red laser pointers, for example, are great tools for presentations and giving your cat some exercise. But did you know high grade laser pointers, preferably green, can be used in astronomy? a well-powered green laser can be used to point out planets and constellations in the night sky.”
https://history.aip.org/web-exhibits/laser/
Maiman developed the first laser that was made out of *pink ruby, which has a high chromium content, and absorbs green and blue light while emitting red light. By flashing white light into a cylinder of ruby, Maiman energized the electrons in the chromium. The energized green and blue wavelengths were absorbed and then amplified the red wavelengths until the light pulse of the ruby was amplified to high power, resulting in a laser. Prior to Maiman’s discovery, physicists had denounced the idea that ruby could work in creating lasers…One of Maiman’s greatest contributions to the field of laser technology was his demonstration of the ease with which lasers could be constructed, making them of great practical use…By 1961, the first commercial laser hit the market. Maiman left his job at Hughes to form a commercial laser company, Quantatron. Laser technology increased as rapidly as the commercial laser industry. Fast on the heels of Maiman’s laser came the dye laser, the helium-neon laser, the semi-conductor laser, the carbon-dioxide laser, the ion laser, the metal-vapor laser, the excimer laser, and the free-electron laser.
https://ethw.org/Theodore_Maiman_and_the_Laser
fun science experiment video, “the uncertainty principal ( Also known as Heisenberg’s Uncertainty principal ) is any of a variety of mathematical inequalities asserting a fundamental limit to the precision with which the values for certain pair of physical quantities of a particle, such an position, x and momentum, p, can be predicted from initial condition.” σxσp=h/(4π)
https://www.thescienceloop.com/2020/09/blog-post.html
Robert Hess, director of holography at Satori Optics, built a lovely vintage laser systems guide from his own collection!
https://sites.google.com/site/vintagelaserarchive/
*Ms. James originally used waves1-5, but this would be confusing to a newbie as we go into wavelength, so ive taken the liberty of replacing it with “product”
product 2– 1969-present,are photepilators, laser-like full spectrum devices…IPL<VPL<BBL
product 3– 1979, as with electrolysis the first use of a laser to target a follicle was ingrown eyelashes, with a market failed argon laser. dermatological use of lasers had noticed hair reduction in treated areas for vascular lesions, and tattoo removal-early animal and human studies started in the 1990s
product 5– 1997-present, in conjunction with cooling systems either cold air or cryo to minimize tissue damage while increasing pulse and power- shooting via diode or using flashlamps with liquid or crystal mediums
https://quackwatch.org/related/Hair/laserhistory/
“in 1998 Andrew and Grossman published the first scientific paper speaking to with results of targeting chromophores for hair removal at Massachusettes General hospital [hair removal state/capital of the world as Gillette and Cynosure are based there]
using a standard normal mode flashlamp pumped ruby, model 936R4H-2, Lasermetrics… A planoconvex sapphire lens (approximately 20-mm focal length) was used to provide a convergent beam at the skin surface and to increase beam coupling into the skin, the saphirre lens was cooled to 4°C to provide heat conduction from the epidermis before, during, and after each laser pulse.
hair loss is fluent dependant, greatest loss is at the highest fluence (60J/cm2)
shaven areas had greatest hair loss, but signifigant hair loss was seen at both shaven and epilated sites vs controls)..
the number of follicles pre and post laser treatment had the same amount, though terminal hair count was significantly lower… miniaturization of the follicular mechanisms“
https://jamanetwork.com/journals/jamadermatology/fullarticle/189173
“ruby provided obvious hair loss in four of seven individuals 1 and 2 years after one ruby laser treatment. In patients with facial hirsutism, repetitive treatments (no. of treatments = 4, mean 61% hair reduction) resulted in significantly better hair reduction than a single treatment (mean 42% reduction) up to 9 months postoperatively…
Three treatments with the alexandrite laser (mean 74% reduction) were more efficient than four treatments of electrolysis (mean 35% reduction) 6 months postoperatively..(overall 55% hair reduction) vs. a single treatment (overall 32% hair reduction)…
Two repetitive treatments with the diode laser (34–53% hair reduction) were superior to a single treatment (28–33% hair reduction)…
NDYAG, Repetitive treatments improved the long‐term treatment outcome with 40% of patients obtaining greater than 50% hair reduction 12–16 months after five treatments vs. 100% of patients obtaining less than 25% of hair reduction after one treatment.”
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1468-3083.2005.01327.
1962: “With Fred J. McClung, Hellwarth proves his laser theory generating peak powers 100× that of ordinary ruby lasers by using electrically switched Kerr cell shutters. The giant pulse formation technique is dubbed Q-switching. Important first applications include the welding of springs for watches.
1963: Logan E. Hargrove, Richard L. Fork and M.A. Pollack report the first demonstration of a mode-locked laser; i.e., a helium-neon laser with an acousto-optic modulator. Mode locking is fundamental for laser communication and is the basis for femtosecond lasers.”
https://www.photonics.com/Articles/A_History_of_the_Laser_1960_-_2019/a42279
“A technique for tattoo removal which produces selective removal of each tattoo pigment, with minimal risk of scarring, is needed. Nonspecific methods have a high incidence of scarring, textural, and pigmentary alterations compared with the use of Q-switched lasers. With new advances in Q-switched laser technology, tattoo removal can be achieved with minimal risk of scarring and permanent pigmentary alteration. There are five types of tattoos: amateur, professional, cosmetic, medicinal, and traumatic. Amateur tattoos require less treatment sessions than professional multicolored tattoos.
Three types of lasers are currently used for tattoo removal: Q-switched ruby laser (694 nm), Q-switched Nd:YAG laser (532 nm, 1064 nm), and Q-switched alexandrite laser (755 nm). The Q-switched ruby and alexandrite lasers are useful for removing black, blue, and green pigments. The Q-switched 532 nm Nd:YAG laser can be used to remove red pigments, and the 1064 nm Nd:YAG laser is used for removal of black, blue, [and grey]pigments… Since many wavelengths are needed to treat multicolored tattoos, not one laser system can be used alone to remove all the available inks and combination of inks.
https://pubmed.ncbi.nlm.nih.gov/11702617/#:~:text=The%20Q%2Dswitched%20532%20nm,%2C%20scarring%2C%20and%20pigmentary%20alteration
Q-switched lasers release highpowered pulses in the range of nanoseconds, which causes the formation
of acoustic waves and photothermal effects that ultimately destroy the tattoo ink particles…a major evolutionary leap in terms of treating tattoos, as well as benign epidermal pigmentary lesions.“a picosecond domain device, producing pulse durations in the trillionth of a second: 10 to the power of -12; therefore, the pulses are 100 times shorter than the Q-switched laser…The picosecond device appears to clear tattoos about twice as fast as the Q-switched nanosecond domain devices.”
http://marketing.cynosure.com/rs/cynosure/images/final%20versionPicoSure_TAG0113_v6_020813.pdf
femtosecond>picosecond>nanosecond>millisecond, laser ablation
“Damage to the material done using femtosecond pulses is perfectly defined for a given material…
two temperature model speaks separately about temperature (kinetic energy) of electrons and of nucleis. Basically it says the following: First electrons absorb the optical energy, and either in a ladder like manner (for longer pulses) or by direct multi-photon process (for shorter ones) are getting out of bound states to continuum. Now two things can happen to the electron:
1. It will collide with a nuclei and transfer its energy to photons (thermalization)After many collisions, nuclei will gain enough energy to escape the bulk
2. Electrons are gaining lots and lots of energy and leave the material (kind of multi-photon photoelectric effect). Nuclei stay cool. But after enough electrons have left, the nuclei remain unbound, and “fly away” due to room temperature energy.
The second mechanism, obviously affects much less area. In fact, being naturally multi-photon, the ablated area is proportional to intensity in the optical spot size in high power, effectively making the “hole” smaller. used in ophthalmology, where the size of the perforation is most critical.
https://www.researchgate.net/post/What_are_the_differences_between_femtosecond_picosecond_nanosecond_and_millisecond_laser_ablation
concerning optical delivery fibers- “Although these wavelengths are within a transparent region of silica glass, radiation of high peak power of the Q-switched laser causes a self-focusing of a laser beam in the silica-glass core due to the non-linear effect of glass, and this sometimes results in damaging the core and end surface. In contrast, hollow optical fibers reportedly transmitted laser pulses with energy as high as 18 MW when the air in the hollow core was evacuated to eliminate air breakdown at the focusing point of the laser beam (Matsuura et al., 2002a; Sato et al., 2000). Hollow optical fibers are also useful for transmitting ultra-short pulses such as pico- and femtosecond pulses.”
https://www.sciencedirect.com/science/article/pii/B9780857092373500047
laser safety guide, with Q&A, has awesome charts to understand wavelength and its penetration, in this case your retina. Safety first!
https://www.lasersafety.com/wp-content/uploads/2017/08/LaserSafetyGuide.pdf
list of lenses needed to protect your eyes based on wave
https://www.phillips-safety.com/2019/05/honeywelluvex-glendale-gtp-laser-safety-glasses-cross-reference-chart/
this has a good explanation of Optical Distance OD rating (OD+2/OD+6/etc.)
https://lasersafetyindustries.com/laser-safety-buyers-guide/how-do-i-choose-laser-safety-glasses/
research done at the molecular, cellular & tissue level showing that low-level laser can significantly increase hair stem cells (https://pubmed.ncbi.nlm.nih.gov/30843235/). No wonder why Low Level (LL) settings of laser can surely stimulate hair growth instead of removing it, but this takes series of repeating treatment sessions for hypertrichosis to happen.”
http://gippslandlaser.com.au/ipl-vs-laser/

^ Ohio State University plastics is running a BBL system, Sciton Forevor Bare BBL.
https://sciton.com/physicians/forever-bare-bbl/
” Long pulse diode lasers ranges from 800 to 810 nm. There are many companies which are manufacturing machines with different wavelength output such as 800 nm, 808 nm, and 810 nm. Among diode lasers 810 nm seems better wavelength as it penetrates deeper and scatters lesser than 800 nm”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4124694/
![20201023_124101[1]](https://kittysbelle.files.wordpress.com/2015/10/20201023_1241011.jpg?w=346&resize=346%2C461#038;h=461 "20201023_124101[1]")
![20201023_124039[1]](https://kittysbelle.files.wordpress.com/2015/10/20201023_1240391.jpg?w=346&resize=346%2C461#038;h=461 "20201023_124039[1]")
^ University of Cincinnati is running a diode, Alma Harmony XL Aesthetic Laser Platform System. “2 IPL handpieces (green and yellow) for vascular lesions, brown spots, red spots, photofascials. SHR handpiece for in-motion hair removal. 2940 iPixel erbium handpiece for skin resurfacing.”
https://www.almalasers.com/clinical-resources/
“It was seen that the percentage of hair reduction after two sessions of treatment was maximum (40%) in the diode laser group, followed by 35% hair reduction in the Nd: Yag laser group and 10% hair reduction in the IPL group. The percentage of hair reduction after four sessions of treatment was maximum (64%) in the diode laser group, followed by 62% hair reduction in the Nd: Yag laser group and 48% hair reduction in the IPL group. The percentage of hair reduction after eight sessions of treatment was maximum (92%) in the diode laser group, followed by 90% hair reduction in the Nd: YAG group and 70% hair reduction in the IPL group.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4477470/
awaiting FDA clearance as of 2019– “Sienna released results from a pivotal trial of SNA-001 involving 65 patients having hair removal with the 810 nm diode laser. After six treatments, hair decreased an average 17.5% with topical SNA-001 pretreatment and laser compared to an average 1.1% in those receiving vehicle and laser. Adding the ready-to-use suspension of silver particles before laser treatment resulted in up to a 32% reduction of light hair compared to baseline, making it statistically superior to vehicle and laser, according to the company.
Researchers also studied SNA-001 in hair removal patients treated with the 1064 Nd:YAG and 755 nm Alexandrite laser. In both cases, study authors reported a significant reduction in light hair from baseline but the difference between patients who received SNA-001 and those who did not in conjunction with these laser devices wasn’t as significant as with the 810 nm diode.”
https://www.dermatologytimes.com/view/help-light-hair-laser-reduction


^Cleveland Clinic is running a Candela Gentle max Pro, which is an alex/NDYAG combo, and it feels sooo good!
https://candelamedical.com/na/provider/product/gentle-pro-series
redheads need a crystal medium laser called Alexandrite (755nm), it favors blonde and red more than diode, reduces the appearance of blood vessels and vascular lesions. finds use in several other fields, including dentistry.
https://www.sciencedirect.com/topics/nursing-and-health-professions/alexandrite-laser
benefits of alexandrite vs diodelasers, though alex and diode are considered “equivelants” in their ability to remove hair, alex favors ginger and blonde hairs slightly better, diode has a slightly higher adverse reaction rate
https://hairfreelife.com/alexandrite-laser-hair-removal-everything-need-know/
“The typical settings employed include pulse durations of 2 to 20 milliseconds, and fluences of 10 to 40 J/cm2“
/dermnetnz.org/topics/alexandrite-laser-treatment/



![20201215_194723[1]](https://kittysbelle.files.wordpress.com/2015/10/20201215_1947231.jpg) ^ aquired handpeices go to a Cynosure Apogee 40 from 1999; the 1mm is used for Telangiectasia (spiderveins), found the 7+10mm, alex safety goggles, box of treatment tips, and a LPIR fiber delivery- set on the right is what im looking for. *the early Cynosure Apogee-alex, Acclaim-NDYAG, and Vstar- dye, all look about the same machine build, but cant verify handpieces match between them all- yet if there’s anything to be learned from videogames, its that generations of machines use the same hardware through out, and sometimes use parts even in between generations, for production cost reduction and platform continuance.
^ aquired handpeices go to a Cynosure Apogee 40 from 1999; the 1mm is used for Telangiectasia (spiderveins), found the 7+10mm, alex safety goggles, box of treatment tips, and a LPIR fiber delivery- set on the right is what im looking for. *the early Cynosure Apogee-alex, Acclaim-NDYAG, and Vstar- dye, all look about the same machine build, but cant verify handpieces match between them all- yet if there’s anything to be learned from videogames, its that generations of machines use the same hardware through out, and sometimes use parts even in between generations, for production cost reduction and platform continuance.
– The red 15mm on right goes to the next hardware generation, an Apogees 6300. keep in mind were delving back 10-20yrs in this vintage handpeice collection build.


^back to interchangeability of handpeices, the aquired 12mm on left goes to an Apogee Elite…pic of the set on the right goes to an Acclaim7000…
a long pulsed ND-YAG (neodymium-doped yttrium aluminium garnet) crystal medium laser, is used to treat black people for hair issues , article covers other medical usage.
https://www.sciencedirect.com/topics/nursing-and-health-professions/neodymium-yag-laser
theres 12 YAG variants for diffrent uses from communication, industry, to healthcare, its the workhorse as it can be doped with diffrent elements in production.
https://en.wikipedia.org/wiki/Yttrium_aluminium_garnet
“The longer-pulse (millisecond) 1064-nm Nd:YAG laser system has been shown to be more effective in safely removing hair than has the Q-switched (nanosecond) Nd:YAG system.
https://dermnetnz.org/topics/ndyag-laser-treatment/#:~:text=Nd%3AYAG%20(neodymium%2Ddoped,medium%20for%20solid%2Dstate%20lasers.
“The results of our study support the safe and effective use of the long-pulsed 1064-nm Nd:YAG laser for long-term epilation in darkly pigmented patients. They also provide information about variations in clinical response at different body locations. Specifically, areas characterized by thinner skin (eg, axillae) were more responsive to laser treatment than those with thicker skin (eg, chin and legs), suggesting that skin thickness rather than hair growth cycle influences clinical outcomes. With thick skin, it may become difficult to achieve adequate penetration of energy deep into the follicle. Body location was further highlighted as an important consideration, as transient pigmentary alteration and vesiculation were limited to areas more prone to sun exposure (eg, face and legs, rather than axillae).
https://jamanetwork.com/journals/jamadermatology/fullarticle/478428
“Lasers that were built subsequent to that seminal paper focused our attention on building lasers that were specific for treatment of certain skin conditions,” Dr. Alster said. “Selective photothermolysis catapulted not only our understanding of how lasers interact with the skin, but allowed us to identify things in the skin that we could potentially target with this new laser technology, and to build laser systems that were specific to those purposes.”
https://www.mdedge.com/dermatology/article/228422/aesthetic-dermatology/experts-reflect-past-50-years-lasers-dermatology



^ aquired handpieces go to a Cynosure Photogenica V-Star, Pulsed Dye laser
sycosis barbae>folliculitus barbae>folliculitus>psuedofolliculitis
“Recent research has confirmed a genetic predisposition to pseudofolliculitis in the African population.” :*(
https://dermnetnz.org/topics/folliculitis-barbae/
keloid treatment options, a pulsed dye laser (594nm) is used for treating keloids formed from Folliculitus Barbae
https://www.youtube.com/watch?v=5aXWZ7sH95U
Laser therapy may be considered medically necessary for the following conditions:
• Keloids or other hypertrophic scars which are secondary to an injury or covered surgical
procedure and either criterion below is met:
Causes significant pain requiring chronic analgesic medication; OR
Results in significant functional impairment
• Mild to moderate localized plaque psoriasis when the following criteria are met
affects 10% or less of their body area AND
have failed to adequately respond to 3 or more months of topical treatments
• Port wine stains and other hemangiomas when lesions are located on the face and neck
https://swhp.org/Portals/0/Medical%20Coverage%20Policies/099-Pulsed-Dye-Laser-Treatment.pdf
^port wine; “CSC-LT (585 nm) resulted in superior blanching as compared to CSC-LT (595 nm). Further study is required to optimize wavelength selection on an individual patient basis during PWS therapy in order to improve treatment results.”
https://pubmed.ncbi.nlm.nih.gov/12430153/
^port wine; “The wavelength of choice is 577 nm, followed by 540, 415, 560, and 500 nm (argon laser). The ruby and Nd‐YAG lasers are predicted to damage the epidermis and dermis at all times when the capillary is coagulated. Concurrent cooling to prevent epidermal‐dermal damage is also recommended here. The CO2 laser is predicted to be the worst laser and, according to our analysis, should not be used to treat PWS.”
https://onlinelibrary.wiley.com/doi/abs/10.1002/lsm.1900060116
Cutaneous Vascular Lesion
17106 Destruction of cutaneous vascular proliferative lesions (e.g., laser technique); less than 10 sq cm
17107 Destruction of cutaneous vascular proliferative lesions (e.g., laser technique); 10.0 to 50.0 sq cm
17108 Destruction of cutaneous vascular proliferative lesions (e.g., laser technique); over 50.0 sq cm
Laser Hair Removal
17380 Electrolysis epilation, each 30 minutes
Diagnosis Code, Cutaneous Vascular Lesion
D18.00 Hemangioma unspecified site
D18.01 Hemangioma of skin and subcutaneous tissue
I78.0 Hereditary hemorrhagic telangiectasia
I78.1 Nevus, non-neoplastic
Q82.5 Congenital non-neoplastic nevus
Q85.8 Other phakomatoses, not elsewhere classified
Q85.9 Phakomatosis, unspecified
https://www.uhcprovider.com/content/dam/provider/docs/public/policies/comm-medical-drug/light-laser-therapy.pdf
Purchasing second hand
“The physician should be aware of the prevalence of different dermatological and aesthetic problems* in the community and then decide which laser would be most suitable for practice in that area. Patients’ attitudes, paying capacity and marketing opportunities need to be assessed. “ [medicaid=poc>pcos>trans]
“The first laser to be bought is a hair removal laser. The wide prevalence of hirsutism, increased awareness among women, and wider acceptance of the technology has made the hair removal laser a necessity.”
“Excimer lamp devices tend to be cheaper than the excimer 308 nm lasers and are quite effective in management of vitiligo and psoriasis. They can be considered as they are cost-effective, effective and safe in dark-skin patients. Pulse dye laser and excimer lasers are expensive lasers, and are found in only few centers ..”
“platform* systems are less robust nor effective as their stand alone counterparts. Stand-alone systems are obviously suited for large practices and established practitioners’ with big budgets, while platforms are more suited for beginners or those with multiple clinics and if different doctors wish to share the machine.”-
*platform system= multiple variant handsets and wavelengths for different procedures
“A large spot size is preferable for laser hair removal.[1] A large spot size allows deeper penetration and allows faster treatments during the laser procedure.”
“Air conditioning is essential for laser equipment as most lasers require an ambient temperature of 18-22° C (64-71 F) for proper functioning. This also ensures a dust-free environment.”
“Cooling: Most lasers require some form of cooling for protection of the epidermis immediately before, during and immediately after a laser procedure. Many devices have built in cooling either in the form of cryogen spray or contact parallel cooling or simultaneous air cooling. It is important to ensure that cooling is working properly to prevent any accidental epidermal injury. Air cooling systems such as Zimmer require regular cleaning of the filter for ensuring optimal performance. Always check the cost of cooling machine and include it in your budget.
“Get quotes from different companies for the similar systems. Pricing depends on the communication skills of the buyer, knowledge of the global and local pricing, discounts offered by the dealer/distributor and the approximate price paid by the other purchasers of the system. It is important to understand that all medical lasers depreciate as soon as they are sold. So getting the best price is more crucial. Always strike a balance between cost and quality while making a decision. “
“A three phase electrical connection is preferred if multiple lasers/devices are being planned. Uninterrupted power supply (UPS) online and offline is recommended and the UPS should be of 3KVA or more with 16 batteries of 60 Amps each.”
“Transportation- taxes can be levied while transporting the machine from the port to the place of installation. Proper documentation needs to be done for this and done accurately. Most of the laser machines are delicate and not supposed to be shifted to various centers. It does affect the life of the machine. Check if such movements can be done.”
Installation should be done from the company representative their self and not by anyone else. It is recommended to know the cost of spare parts from the parent organization, well in advance; this is helpful for the future course of action. An Annual Maintenance Contract is essential for insurance purposes. Many insurance companies offer additional electronic insurance that may be cheaper than the AMC offered by the laser companies after the warranty period is over.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4134647/
“laser technology will continue to improve and new systems will be introduced that will affect both the quality and the cost of health care delivery. Striking the correct balance between quality and cost under the realities of the prospective payment system has added a new twist to the capital equipment, decision-making process. In this cost-quality equation, the purchasing manager figures prominantly, for a properly negotiated capital equipment contract can reduce both short and long-term operating expenses, and thus increase return on investment. As the resident expert in contract negotiations, therefore, the purchasing manager is a logical choice to any team selected by administration to evaluate the merits of a piece of laser equipment.”
https://pubmed.ncbi.nlm.nih.gov/10274491/
“Many pre-owned and refurbished cosmetic laser equipment outlets, warehouses, and brokers can refer you to dependent third party technicians in the industry. Many times these technicians can come to your practice and fix your machine on the spot rather than having to ship and insure your machine. These third party companies can service and repair your cosmetic laser machines for a fraction of the manufacturer’s price, up to 75%.”
https://www.linkedin.com/pulse/repairing-your-medical-laser-what-you-need-know-ari-marom
Cynosure
https://www.cynosure.com/for-providers/
summarized phone call on 7/31/20 at 2pm..
1- The Cynosure, Elite HQ* surpasses the former 18mm spot size advantage of the Elite+,by increasing its treatment range from two to twenty-four mm handpieces. Giving it the fastest treatment times available.
Elite iQ™ Aesthetic Workstation Skin Treatment – Cynosure
2- In keeping with Cynosures history of advancements in laser technology, they have produced and patented the only objective, Skintel* melanin reader, to ensure accurate perception of abundance between clients. Ensuring use of the safest levels, therefor the most effective treatment available a person of color.
Skintel Melanin Reader – UK Physicians
3- The Elite iQ has more power than its closest competition, the Candela Gentle Max; by 18% Alexandrite, and 43% ND-YAG. Increasing each passes reduction rates. Making it the most effective laser specialized toward hair removal on the widest range of skin types.
4- The Elite models do not need any “upkeep” as with some other lasers; there are older Apogees’ produced 20 yrs ago in the field still operating strong. Though an optional annual warranty in the range of 5k ensures it against any failure.
5- Cameron Colby, Our Tri-State areas Cynosure sales rep, would like an opportunity to come in and speak face to face with those involved in the finale decision making process.
He was found to be attuned to our needs in specializing treatment to minority clients.
Final price along with references to physicians currently operating Elite IQ and Elite+ models in Ohio, will be discussed at this meeting.
Cameron Colby
Cynosure Area Sales Manager, TN – KY – OH
603-833-0820
cameron.colby@hologic.com
We are able to build a vintage laser bay to shoot in your basement for $____
Alexandrite
The Apogee40, was released in 1999,,1.5k, Alexandrite replaced Ruby and allowed red-heads and blondes to see benefit from treatment.This model has fiberoptic delivery, but no handpeices, but found some 🙂
*ha! now theoretical laser tech level, whose able to treat light-brownish-redish-blonde better than UC or OSU 😛
Apogee5500, alex, 2004
Apogee6200, alex, 4k
Apogee9300, alex, 2003-2009, negotiable 3,400-20k
Apogee+, alex, 20k, 2012 (like the black accents)
Apogee Elite, alex+NDYAG, 2,900 up to 20-40k,is the original “blend” of laser hair removal therapy; not only combining both the Alexanderite and NDYAG in one machine but giving the ability to shoot both wavelengths at once! This is now industry standard, which allows treatment to be tuned specifically to each individual client.
elite, ELMD,2006-2007, (sought after by laser wholesalers) plus sexy with the glass top 😛
Accolade, alex, qswitch, 2008, 1.7k (is a neat blue color an so are the handpeices)
elite, ELNL
elite+
elite mpx, 28.5k, 2011
MDX models (15k-30k), 2007, added the familiar IPL alongside alex/ndyag
elite IQ
ND-YAG
Photogenica V, pulsedye, 1996, 500, all lasers afford some treatment, diy-ers go!
Photogenica V-star, Pulse Dye, 2001, 2k,
Photogenica SV, pulsedye, 2002, 1000
Acclaim 6200, NDYAG, , 2k,
Acclaim 7000, NDYAG, 1999, 1-5k, this model has no delivery, handpieces, and “missing a panel”, but looks like it uses the same delivery and handpieces as the Apogee40, worth fixing if it still has a crystal (pulling the rods in each machine originally listed in this section is worth more than asking price.)
Acclaim 9300, NDYAG, 1999
Cynergy, pulsedye+NDYAG blend combo, 2006-2007, 12-20k, this is what you want as a patient specifically facing keloids, look for centers and ask for this machine. see Elite+ for hair removal
all lasers can be serviced, and must be, before you use them in an insured medical environment.
Candela acquired Syneron, whose products still claim 30% of the medical laser market. A precursory look finds more people working on candela than people selling parts or machines, telling me this is top of the line for 2019 as they are all still in service. Also pricey, a handpiece to a gentle max pro is 1,500+.
Alex-1, alexandrite, 2001, 15k (so cute how big the handpeices are!)
Mini Gental Yag, ND-YAG, 2004, 14k
GentleLASE, , 2007, “gentle” tech is the use of cryogen instead of cold air, so while it feels better to the patient it adds disposables to continued operation (so worth it though)
GentalLASE plus, alexandrite ,15k
Gentle Max, , 2013, 39-65k (sought by dealers)
Gental Max Pro, alexandrite+ND-YAG blend combo, top of the line for hair removal 2019
TJS services and supplies parts for the candela gentle max
https://www.tjslasers.com/laser-repair/repair-medical-lasers/candela-flash-lamps
candela error codes
https://laserpartrepair.wordpress.com/candella-error-codes/
Cryogen tanks, are 325usd, for a box of 12 cans, at 1000grams each, “the old reusable cryogen cans for the Candela lasers are refillable, unlike the new cans.
https://laserscientific.com/product/cryogen-for-all-candela-lasers/
Laser Warehouse, services the candela gentle max, and cynosure elite
https://thelaserwarehouse.com/cosmetic-laser-repair-service/cosmetic-laser-repair-brands/
“how to get laser hair removal covered by insurance”
http://www.huffingtonpost.com/monica-leftwich/how-to-get-laser-hair-rem_b_8169606.html
- I went to a dermatologist
- Procedure Code Identity: 17999(I found this atwww.acgme.org/acWebsite/downloads/oplog/080byAreaType.pdf)
- Description of Service: laser hair removal
- Diagnosis Code: 626.9 (PCOS code)
http://www.soulcysters.net/showthread.php/236666-My-Insurance-is-Covering-My-Laser-Hair-Removal!
“..But the blurbs say that if you use a “”99” code the insurance will want the Dr. to justify the medical need. (Although there is a clear medical need as removing a beard for a woman is not just cosmetic.) The Dr’s office told me that they don’t know of a code! So I am sure that if they did not wish to look up a code, they will not wish to print a letter of medical necessity to justify insurance payments. I was, therefore, looking for a non-general/non-99 code.“
ICD-9-CM 704.9 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, 704.9 should only be used for claims with a date of service on or before September 30, 2015. For claims with a date of service on or after October 1, 2015, use an equivalent ICD-10-CM code (or codes)
http://www.icd9data.com/2015/Volume1/680-709/700-709/704/704.9.htm
“If there was a lawsuit, then I suspect the name of the plaintiff is not private and her privacy would not be implicated if her name was revealed to you by CareSource.”- truth is caresource refuses to give me any more information. [and i cant find it so they settled on a singular case. i traded my own for everyones access]
https://www.avvo.com/legal-answers/a-trans-woman-in-ohio-took-her-medicaid-to-court-a-3083862.html?utm_campaign=answer_notify&utm_content=question_legal&utm_medium=email&utm_source=notification
Transgender Law and Policy Institute, a wealth of law, cases, resources on anything from immigration to employment, has guidelines and resources for enacting law and policy (look further into)
http://www.transgenderlaw.org/resources/index.htm
word of mouth. “As far as I know, a doctor has to refer patient to an Electrologist, then we fill out a form and the client takes it back to their doctor to be filed with insurance. The insurance code for electrolysis is different from the laser treatment code…… I just attended the AEA conference in Rhode Island. When I asked, that’s the information I was given. Electrologists – from what I was told – Electrologists are not medical professionals as far as insurance is concerned, so we can’t file the actual claim to insurance companies. I’m still working it out, so all I have to offer is that information that was just given to me a few days ago. It might even be different for each state, I just don’t know.- Last January President Obama issued an order mandating that plans under the ACA cover medically necessary care for transgender persons. Since all plans participating in ACA exchanges must offer the same services, this means that for the vast majority of employer plans, all medically necessary transgender related services would be covered. But the challenge is that not all states participate in the ACA at the same level, and each plan determines how it meets the medically necessary criteria. What you need to find out Jaiowyn is if there are any electrologists affiliated with your particular plan. For example, Kaiser in Southern California has a list of a dozen or more electrologists “on the list” Your PCP may not even know if this list exists. You should contact member services, find out who coordinates services for transgender clients (I doubt your the only one they’ve dealt with,) and ask that person about hair removal. What we’re finding is most plans are readily covering pre GCS hair removal,facial not so much.”
[ok. so gota build a legislative team first?]
 Been trying to become an electrologist in Ohio for a number of yrs and have researched it to the extent we could call it “purposeful and systemic barriers”, enough to be able to explain the “job security” measures adopted by the
Been trying to become an electrologist in Ohio for a number of yrs and have researched it to the extent we could call it “purposeful and systemic barriers”, enough to be able to explain the “job security” measures adopted by the Electrolysis Cosmetic Therapist Association of Ohio, legislated into law by democrats, amended by republicans, enforced by the DoH in Columbus whose only reference to the field is the Association, DoH has no committee and relied solely on that Associations co chair who’s currently practicing charging 140 dollars an hr in the field.. the requirement of 150 hrs of head and neck massage that no electrologist ever uses and that no school in the world consider outside of ohio, leaves those who own for profit schools as gatekeepers to who enters this entirely proprietary field- with training that prioritizes salon owners over the individual technicians.
in the 60s and 70s there was a move legislatively to close up these feilds, being successfull to various degrees in 2/3rds of the states, whether that was for their donors business interest or a genuine concern, is perceptional.*insert the safety dance video
“Mr. Artinian, whose electrolysis school is one of the largest in NY ,“I’d be in favor of legislation as long as the require ments were fair and not designed to keep people out,” he said.
Masha S. Wise, recording secretary of the Association of New York State Electrologists, said the main aim of the 100‐member group was licensing and “improving the education of electrologists.”
“In the best of hands, electrolysis is a problem,” said Dr. Norman Orentreich, who is associate clinical professor of dermatology at the New York University School of Medicine.He is particularly Incensed at the instruments sold for home use (“it’s criminal to do it yourself”) and believes that a “responsible” society would have a method of determining ability before allowing operators to treat people.”
Garo Artinian, director of the Kree Institute, was discusing the opportunities offered by a career in electrolysis. “Any girl with a nice per sonality can make herself $300 to $400 a week as an electrolysis operator. It’s as easy as falling off a log,” he said.
Mrs. Joseph said. “For our own prestige and for public safety, we feel it’s an absolute must to attain licensing. As it stands now, anyone can buy equipment and practice…. there are no controls.”
However, Mario Bellardi, general manager of the Hoffman Electrolysis Institute, said that licensing is not the answer. “As soon as you get licensing in anything. you get involved in politics,” he said “Things should be left the way they are. If an electrologist is not doing the work properly, he or she won’t be able to stay in business.”
https://www.nytimes.com/1971/02/27/archives/the-great-electrolysis-debate-should-operators-be-licensed.html
“Come visit New York and go home with a new career!” (The Kree Institute had a 90-hour program of electrolysis training.)-mike bono, [NY to this day remains an unliscenced state]
https://hairtell.com/forum/t/electrology-history/40307
Montana fell prey to this movement in 1981, which in part was due to the “electric tweezer scam” and part due to advancements in microbiology and understandings in germ warefare.
“DONNA ALlRES, an electrologist from Kalispell, ;testified that her main concern was for the safety of the public. She felt that without licensing there could be a spread of communicable disease because a physical exam would not be required. She stated that, even to give a manicure in that state, one must be a cosmetologist.
KATHRYN (KATIE) TUCKER, member of the Board of Electrology, testified in favor of the bill, but did propose an amendment to it. Tucker’s proposed amemdment to the bill would require that all individuals performing hair removal by other than the electric needle be required to have the background and training of a cosmetologist in the study of skin textures and hair or require that the hair removal be performed only in a licensed cosmetology establishment under supervision of a licensed cosmetologist. She said the board also intends to have a “grandfather clause” to allow those to practice who have prior to enactment of the law.
CAL CAMPBELL, representing the Montana Department of Health and Environmental Sciences, Food, Drug and Cosmetic Section Supervisor, testified as a proponent. He was called into the controversy as a result of receiving complaints because of the non-permanent nature of the tweezer hair removal.
REP. PAVLOVICH asked if an electrology operator must go to a beauty school. ARTHUR said an operator had to go to an electrology school, most of which require 500 hours of training, in addition to being a trained cosmetologist.
REP. BARDANOUVE asked why a grandfather clause should be included. TUCKER, of the Board of Cosmetology, said that was for people who were already in business.
http://montanacourts.org/Portals/189/leg/1981/house/02-18pm12-hhs.pdf
“Upon the formation of a state board, “grandfathering” in of certified or non-registered Electrologists would be most unwise, resulting in a confused mess of differing standards, and in no change to the lack of professional competency for the most part…in 1996 the FDA upgraded electrolysis equipment to the status of a class one medical device.“
https://www.bostonschoolofelectrolysis.com/article_41.php
“You will never find anyone in your area to train you, they look at it as inventing your own competition, and therefore giving away their own earning potential. I seriously have people who think that me treating someone in Buffalo NY is taking money away from her in, say, North Carolina.”- james walker
https://hairtell.com/forum/t/help-me-please/30040/13
school for electrology
its like they’ve created this wall. Here is the contact information for the 3 schools that can train for Ohio:
- About Face Cosmetic Therapy, owned by Vickie Mickey (Kay told me this is the school that would fight me fixing electro’ stuff in ohio, as vickey is the one who put in the massage requirements; though vickey herself claims they were already there?)
she wants 18,500 and that licenses me as an cosmetic therapist
1918 Bethel Road, Columbus, Ohio 43220
By Phone: 614-457-0448
By E-Mail: aboutface@aboutface-ctc.com
http://aboutface-ctc.com/laser-hair-removal-instruction/ - Ohio Medical Electrology Institute
attn. Jo Melching (heard she would be more sympathetic to the plight of a fledgling electrologist) speaking with her she would be willing to apply to accept federal loans if somone was willing to do the taxes and fees for her. her classes are (were16,000) now 18k,*now 15k due to covid
271 Cline Ave. Suite # 4
Mansfield, Ohio 44907
419-747-7546
e-mail:jomelch1@aol.com
or visit: http://www.skinsolutionsandelectrolysis.com/ - one in ky (also 2 hrs away) does have 3 different levels of courses, i could do 350 hrs that wouldn’t license me in OH but it would elsewhere but nowhere i wanna go. would give me a better understanding of what im doing to myself. This seems like the most ethical route for ohio liscensure, as they had to fight Ohio too.
http://bgskincare.com/main/school/?page_id=62
350hrs: $5,100
600hrs: $6,800 (according to Amy Day, this matches the price of the last feasible school that existed in ohio that she herself went too.
765 HOURS: $10,000- 9 months of schooling, some can be done online some in a formal setting. 5k upfront, and 5k by end of the semester. This meets Ohio’s requirements to pass a state exam, KY itself has no licensing requirement whatsoever, this course was developed by interviewing Ohio graduates to find out what was even on the exam to be taught. eventually gaining ohio acredidation “8-9 yrs ago” meaning 2010-2011-2012-ish they gained ohio medical board aproval- they have programs for veterans, so are accredited with anouther fed training program.
Laser Hair Removal Courses: We also offer Laser Training courses which can be completed in one week or less.
30 HOURS: $2600.00 (Three day course)
50 HOURS: $3500.00 (Five day course, one week from Monday-Friday)
http://electrologyinstitute.com/
for context; 1/3rd of the states in the US have no liscensure requirement whatsoever. for those that remain anywhere from 350-1100 hrs, now Ohio might seem to be right around the average of 750hrs- but in reality its the worst state to try to get accredited. the laughable requirement of 50 hrs of head n neck massage that no electrologist in the world uses, on top of the 600hrs of electrology, is baring people from entering the field. Massachusetts and New Jersey have the highest of 1100hrs, can accredit for anywhere in the world but Ohio, they dont teach “massage therapy”-they teach electrology.
this pdf is ohios licensing requirements
https://professionals.electrology.com/be-an-electrologist/electrology-licensing-requirements.html
this is information of how many were practicing befor the 92 corruption
CT rule info and Stats 1992
this explains how many were expected to be destroyed in 1993
Effects of Sub HB 322 on CT
this is how many we have left as of 2019
CT roster May 2019
we lost 3/4th of the feild of electrology in ohio, this including 26 yrs of “regrowth”
Friend tried to help me address the systemic issues… but never heard back from the state reps they contacted.
(Aaron)
“Good morning Jim,
Sent this to Representative Butler this morning:Had an individual pose a question to me that I believe you might be able to help find answer. OAC 4731-1-07 requires that to become a licensed electrologist in Ohio you must attend a school based in Ohio, surround State’s licensures are not acceptable. The catch with this restriction is that NO SCHOOL currently exist in Ohio from which to obtain training. Ohio Means Jobs show 1380 currently employed electrologist with an expected growth of 30 for the year. How is this obtainable when there is NO training pathway? Follow on question would be WHO benefited when restriction was put into place? Excerpt from OAC 4731-1-07 is included below.
Thank you kindly and anticipate your response.
Respectfully,
Aaron
4731-1-07 Eligibility of electrologists licensed by the Ohio state board of cosmetology to obtain licensure as cosmetic therapists pursuant to Chapter 4731. of the Revised Code and subsequent limitations. -A person who was issued a cosmetic therapist’s license prior to February 1, 1993 based upon holding a certificate to practice electrolysis and registration issued under Chapter 4713. of the Revised Code, may be registered by the board as a cosmetic therapist but may not apply “systematic friction, stroking, slapping, and kneading or tapping of the face, neck, scalp, or shoulders” as defined in division (A)(2) of section 4731.15 of the Revised Code until that person has completed coursework in that area that has been approved by the board at a school approved by the board pursuant to this chapter of the Administrative Code.”
Also sent to Representative Strahorn (Minority Leader) and Representative Rosenburger (Speaker of the House)
Jeff
“Aaron, Thank you for the email. I reached out to a contact I have at the Medical Board to see if he could possibly shed some light on the situation and provide some answers. I just emailed him a few minutes ago, so I haven’t heard back yet, but I will share his response with you when I receive it. Thanks again for writing, and hopefully we can get a good answer…
Best Regards,
Jeff Dillon
Legislative Aide
State Representative Jim Butler, 41st District
77 S. High Street. 13th Floor / Columbus, OH 43215
Office: 614-644-6008
Fax: 614-719-3591
Email: jeff.dillon@ohiohouse.gov
did try to insert myself into the 2020 barbering bill concerning deregulation, in reality the push to deregulate by republicans is a way to separate democrats from their donors in a sychotic self harm as their both wings of the same bird just as guilty, yet neither side should of ever of let someones money sway their legislative hands.
HB-133 proponnent testimony (1)
“COLUMBUS- State Rep. Thomas West (D-Canton) today announced that House Bill (HB) 442, his bipartisan bill with Rep. Bill Roemer (R-Richfield) to enact Certified Public Accountant (CPA) licensure reform, has cleared the legislature after the House concurred Senate amendments. The bill now moves to the governor’s desk to be signed into law…is a student-friendly bill that makes the process of taking the CPA exam more flexible for aspiring CPAs. This simple change will make Ohio more competitive and a better place for these students to study and ultimately work…The Senate Transportation, Workforce and Commerce Committee did accept an amendment to HB 442, which implemented various occupational licensing reforms recommended by the House State and Local Government Committee in its December 2019 Occupational Licensing Review Report.
https://ohiohouse.gov/news/democrat/rep-wests-bill-to-reduce-hours-required-to-sit-for-cpa-exam-moves-to-governors-desk-104888
holy shit, I just deregulated the hardest state in the nation to work in- we are now an unliscenced state O.o
“On January 7, 2021, Governor DeWine signed House Bill 442 into law. A number of the statutory changes will impact State Medical Board of Ohio licensees.
Cosmetic Therapists
• The license requirement for cosmetic therapists in Ohio has been eliminated. Cosmetic therapists will no longer be licensed by the Medical Board or any other licensing entity in Ohio.
• A definition of cosmetic therapy has been added to Ohio Revised Code chapter 4713, which regulates the Ohio State Cosmetology and Barber Board. The revised chapter indicates that an individual may provide cosmetic therapy in a salon if authorized by the Ohio State Cosmetology and Barber Board.
Massage Therapy
• The amount of education hours required to complete a massage therapy program will be reduced from 750 to 600 hours. The amended education hours must meet the minimum requirements:
o Two hundred seventy-five hours in anatomy and physiology and pathology;
o Two hundred seventy-five hours in massage theory and practical, including hygiene;
o Twenty-five hours in ethics;
o Twenty-five hours in business and law.
Physician Assistant
• Changes in the law will now allow the Medical Board to recognize any accrediting organization for physician assistant education programs. Previously, the board required physician assistants to be accredited by the Accreditation Review Commission on Education.
https://med.ohio.gov/Publications/Recent-News/house-bill-442-changes-to-ohio-law
the cosmetic therapy associations responce video [use the wayback machine as its been removed]
their freakn out an so am i! in it states: “its easier to change rules than legislation, there was no need to move us from medical, all they had to do was change rules concerning requirements…they will continue to work with DoH who will continue to oversee laser…for our own prestige…may yet turn this to our advantage…they watched the proceeding videos and know who i am.”
https://www.youtube.com/watch?v=88B0nkHlgkk
“The fallout from Ohio House Bill 442 has unlicensed Cosmetic Therapists and removed our schools from being regulated by the State Medical Board of Ohio (SMBO). As SMBO is the only reason why we have been allowed to perform laser hair removal there is a concern that if the Cosmetology and Barber Board (CBB) becomes the regulating body for our schools that they will not support our capability to retain this. The main reason why we want to avoid CBB being involved in our profession in any way is because lasers, and electrolysis machines for that matter, are medical devices. We are aware that CBB has not allowed Estheticians to use Microneedling machines because of their designation as a medical device. Also, Cosmetic Therapists were once regulated under CBB in past decades and they supported our move to the medical board for the reasons shared above. Our first step to protecting our profession is to get laser hair removal added to our legal (statute) scope of practice. That would ensure that no matter what board regulates us at any point in the future, that we would have a legal right to run lasers. Right now we do not have this added protection the way our current scope is written. Although this will not give us full autonomy on running lasers without doctor supervision, it will set us on the path to make that argument in the future when laser rules come up for review. Speaking of rules, in December 2020, the medical board discussed expanding what a Cosmetic Therapist could be allowed to do with lasers other than hair removal. This was a long time in the making. CTAO has spent the last decade repairing our relationship with SMBO. This was proof of our success and that they trust us. Dr. Bechtel, who is one of the highest respected Dermatologist in the state and the current President of SMBO, stated “that vascular lasers are probably the safest of all lasers and have a lower risk of scarring, and that is why the vascular laser was chosen for expansion into the scope of practice of nurses and cosmetic therapists.” He also went on to say “while allowing cosmetic therapists to use laser for tattoo removal may be something the board could consider in the future, it is not included in the current proposed rule…”. If our schools are removed from their regulation, it’s possible they could reverse their standing on expanding our capabilities due to them no longer being involved in our education standards. Without a state board licensing examination that has now been eliminated, SMBO could still adopt rules regarding what the school’s final examination of competency to practice and the score that constitutes evidence of passing. We believe giving SMBO this regulation will encourage them to continue to see us as a valuable asset to the medical industry, even as an unlicensed profession.
CTAO has decided to work with The Buckeye Institute and ask for their help in getting laser added to our legal scope of practice and to get our schools reinstated under SMBO for regulation. If you agree on this course of action, please sign this petition. [signed]
https://www.change.org/p/the-buckeye-institute-add-laser-to-cosmetic-therapist-scope-of-practice-retain-smbo-to-regulate-our-schools
 So of those electrologists in Ohio, half wont even work on a trans person, of the half that do some prefer we come in “after hrs”, and most refuse to do pre-op work for surgery. Trust is paramount when talking about an estimated 65 an hr at an est 100-400 hrs to clear a face. Its an insurmountable cost to a minority known as THE health disparity population, yet no-one is seeing us as projects to be done but perpetual clientele effectively leaving those most in need of the fields services without access to it- ensuring were “left visible and thus vulnerable”.
So of those electrologists in Ohio, half wont even work on a trans person, of the half that do some prefer we come in “after hrs”, and most refuse to do pre-op work for surgery. Trust is paramount when talking about an estimated 65 an hr at an est 100-400 hrs to clear a face. Its an insurmountable cost to a minority known as THE health disparity population, yet no-one is seeing us as projects to be done but perpetual clientele effectively leaving those most in need of the fields services without access to it- ensuring were “left visible and thus vulnerable”.
update 2018- Equates is run by TERFs, an their protecting the cosmetic therapy association who instituted the insane job restriction barriers on those able to practice in Ohio. for verification all you need to do is look at their employee roster and realize they picked up Karla Rothan from stonewalls Columbus pride, who we had removed over the police brutality of black pride 4. worthy of note when i meet her infesting Equates she told me to “just move”, in response to why Equates refuses to actually cover trans healthcare according to its makeover grants requirements. You cant even get case management unless you have aids but were high risk enough that we cant sell plasma? Lets not even get into personal discrimination through Bravo/equality ohio, another fake LGB-t org tied up with Equates.. Anyhoo, that’s why you wont find me allowed to speak at the TransformingCare Conference, because its not about trans healthcare but enforcing the status quo.
at OSU when i originally presented this work in a PowerPoint i turned down Mike Bonos offer to do my work as this wouldn’t have been a repeatable process, i would of got it done but noone else would; there would be no clinic built, no help with licensure, no help against the state, and noone seemed concerned with access of the impoverished right here in Leelah Alcorns’ graveyard. soon afterwards i would prove discrimination from Caresource to medicaid oversight, winning us all laser coverage.
https://www.teenvogue.com/story/ohios-black-pride-4-were-arrested-at-the-stonewall-columbus-pride-festival-and-parade
while the restrictions on the feild are legislative and therefor must be undone legislatively, the DoH of Ohio is also harming trans patients by refusing to allow correction of a birth certificate which outs us in any background check; trans people can be denied bank accounts, insurance, even have their water shut off due to an incongruity on forms. job and Family Services BTW are acting contractually illegally by using gender on a BC which is a secondary document, ignoring the F on our state ID and passport (without having to fight a lengthy appeal process.) hence denying access to sustenance, proper housing, and work programs.basicly what im saying is the state is already required to recognize our gender identity.
https://kittysbelle.wordpress.com/2017/12/28/jfs-discrimination-appeals/
ACLU in ohio is under pressure from the national org to perform in areas they dont want to win.
which is why i cant find representation for a case of discrimiantion from state resources over a BC spanning 4 counties and a decade; as they have won an amendment, not a correction.
https://kittysbelle.wordpress.com/2019/07/23/a-decade-of-discrimination-from-job-and-family-service-programs/
^ which will still out us in any background check whatsoever, its considered a C grade.
https://www.lgbtmap.org/equality-maps/identity_document_laws
meanwhile equality ohio is pushing a hidden RFRA derived of 2 lesbians from franklin county willing to barter our rights for equal partner benefits, guised as a “fairness act”, in its original incantation didnt cover trans people, that as designed from the start will take away caselaw instituting a “process of mediation” eventually known as religious arbitration.
https://kittysbelle.wordpress.com/2015/12/01/religious-exemption-or-the-rules-dont-apply/amp/
just so you know that legal social services don’t exist.
transphobic mindsets exists in some form or another within most large receptions staff pools- the first person a trans patient contacts when trying to get care… as well vetting proper referrals by you and your well trained staff is a must.
https://www.them.us/story/transphobic-voicemail
7 tips for surviving the drs visit as an intersex person
https://www.youtube.com/watch?v=B-ihx4l5qGI&feature
“[The barbershop is] a neighborhood hub,” she says. “It’s where a lot of people go to just share information, and you can’t do that if you’re ostracizing certain demographics.” At her last barbershop, she found that creating a safe, nonjudgmental haven via her chair became a juggling act. “There were, in my opinion, a lot of side comments that were homophobic and transphobic in nature. There were a lot of comments that came off really misogynist and sexist,” Dez said. “And for me, it was a balance. Because one, I was trying to create a safe space for my community, within a safe space for another group of folks.”
https://www.teenvogue.com/story/transgender-haircut-salon-experience?verso=true
mental health disparity’s
2 large federal studies were done, one in 2011 titled injustice at every turn
https://endtransdiscrimination.org/PDFs/NTDS_Report.pdf
and anouther follow up in 2015, both showing we own the stats of discrimination and abuse in every realm imaginable (we are the minority in every other)
https://www.transequality.org/sites/default/files/docs/USTS-Full-Report-FINAL.PDF
* Expecting Rejection: Understanding the Minority Stress Experiences of Transgender and Gender-Nonconforming Individuals
http://online.liebertpub.com/doi/full/10.1089/trgh.2016.0012
http://www.medscape.com/viewarticle/868818?nlid=109352_2051
^ an interview with Brian Rood: Expectation of rejection makes people who are transgender feel anxious, isolated, depressed
https://www.minnpost.com/mental-health-addiction/2016/10/brian-rood-expectation-rejection-makes-people-who-are-transgender-fe
Why Transgender People Experience More Mental Health Issues, It has nearly everything to do with the way they are treated. Psychology Today
https://www.psychologytoday.com/blog/the-truth-about-exercise-addiction/201612/why-transgender-people-experience-more-mental-health
Protecting Transgender Rights Promotes Transgender Health
https://lookaside.fbsbx.com/file/trans%20rights%20and%20trans%20health.pdf?token=AWw9nYEE99gDF-mtxKHdCOrn8JyxI1Q8aPy5j6CRGqrMn5Np4b5Ep5wPCY0ZTQNG9QnLUE8mTCNtPc6UhjCNbqn-CRl93mvu0SB_qU_bFtH1fC7Ea7mjLMXxV_qUtqGZjLwTPtIGBFq3GdAtjvyR9oCs
employment
the financial penalty for being transgender in America
http://www.lgbtmap.org/unfair-price-transgender
what employment discrimination is like for trans people
https://www.buzzfeed.com/chrisgodfrey/this-is-what-workplace-discrimination-is-like-for-transgende?utm_term=.loEyVoxJK&bftw=lgbt#.ig9d26PzW
feeling helpless as the business world tears down my transgender wife
http://transgenderuniverse.com/2016/12/21/feeling-helpless-as-the-world-tears-down-my-transgender-wife
3 trans people speak of the horrific struggle of finding a safe and supportive workplace
https://www.bustle.com/articles/200589-3-trans-women-share-their-horrific-struggles-to-find-safe-supportive-workplaces
transgender law centers example pdf concerning employment
http://transgenderlawcenter.org/issues/employment/modelpolicy
for the employer
http://www.workplacefairness.org/gender-identity-discrimination
creating a LGBT friendly work environment
http://cms.bsu.edu/-/media/www/departmentalcontent/counselingcenter/pdfs/safezone%20out%20at%20work/creating%20an%20lgbt-friendly%20workplace.pdf?la=en
Workplace Gender Transition Guidelines at Berkeley Lab
http://diversity.lbl.gov/resources/gender-transition-guidelines/
AU transgender people and work, a guide for Victorian employers to help integrate Transgender people into the workplace. It outlines what “Transgender” actually is, and gives guidance on making sure Human Rights Laws aren’t breached.
http://www.genderqueer.org.au/transgender-people-at-work/
advocate talks about how your business can be trans inclusive
http://www.stevenspointjournal.com/videos/news/2016/10/18/92386658/
Medical health disparities
NIH declares LGBT people as health disparity population
http://www.washingtonblade.com/2016/10/06/nih-designates-lgbt-people-health-disparity-population/
Lancet medical journal releases need for transgender medical competency
http://www.thelancet.com/series/transgender-health?utm
“trans broken arm syndrome”
http://transgenderuniverse.com/2016/06/16/trans-broken-arm-syndrome/
a comic about the “awful double standards for hormone treatment between cis and trans”
http://everydayfeminism.com/2015/09/hormonal-treatments-cis-trans/
MedicalXpress, Transgender patients discriminated against for health care services
http://medicalxpress.com/news/2014-02-transgender-patients-discriminated-health.html
medical students have to push for more LGBTI training
https://www.gaystarnews.com/article/med-students-push-for-more-lgbti-health-training/#gs.LnBHvM6j
A survey by the Royal College of Nurses has found that more than half of nurses have cared for transgender patients, but only 13% of them felt prepared to do so.
http://www.medicalwebtimes.com/read/is_health_service_transgender_friendly/
a trans learning gap in the ER
https://www.nytimes.com/2017/04/13/well/live/a-transgender-learning-gap-in-the-emergency-room.html?_r=0
embracing the benefits of reassignment surgery, a need for surgeon training programs
http://www.kevinmd.com/blog/2016/10/time-embrace-known-benefits-gender-confirming-surgery.html
assessing access to care for transgender and gender nonconforming people: A consideration of diversity in combating discrimination
http://www.sciencedirect.com/science/article/pii/S0277953614002111
8 pdfs used by the CDC
https://npin.cdc.gov/stdawareness/lgbtresources.aspx
endocrinologists want training on how to treat transgender patients
https://www.insurancenewsnet.com/oarticle/endocrinologists-want-training-in-transgender-care
study shows trans adults have higher risk for poor physical health
https://www.gaystarnews.com/article/study-trans-adults-in-the-us-have-higher-risk-of-poor-physical-health/#gs.7dzvtr
A new *gay only* study “of both patients and providers in JAMA Internal Medicine looked at the feasibility of gathering such information in emergency departments. Nearly 80 percent of providers surveyed believed that patients would refuse to disclose their sexual orientation. By contrast, only 10 percent of patients from a randomized, national sample of lesbian, gay, bisexual and heterosexual subjects said they would refuse. (Those who said they would decline were more likely to be bisexual.)”
LGBTQIA2 people are hesitant because its about safety and continued access. consider now being outed as trans by your documents or 5 o’ clock shadow, how dangerous could such an everyday occurance eventually get? and what does that do for ones self image unable to to do more than cry to the heavens over an otherwise readily treatable malady.
https://www.nytimes.com/2017/05/29/health/lgbt-patients-doctors.html?smid=fb-share&_r=0
Unraveling Injustice: Race and Class Impact of Medicaid Exclusions of Transition-Related Health Care for Transgender People
http://www.deanspade.net/wp-content/uploads/2010/08/gehiandarkles.pdf
“The fact businesses … aren’t making it a priority to ensure women of color receive the same level of treatment a fair-skinned woman does speaks volumes about how little they value us as clientele,”
https://www.racked.com/2018/6/2/17419236/people-of-color-black-people-laser-hair-removal
UCLA study finds transgender adults more racially, ethnically diverse, of course, we are the minority within every minority..
http://dailybruin.com/2016/11/02/ucla-study-finds-transgender-adults-more-racially-ethnically-diverse/
“Pseudofolliculitis barbae (razor bumps) is a common condition of the beard area occurring in up to 60% African American men and other people with curly hair. The problem results when highly curved hairs grow back into the skin causing inflammation and a foreign body reaction. Over time, this can cause keloidal scarring which looks like hard bumps of the beard area and neck. Shaving sharpens the ends of the hairs like a spear. The hairs then curve back into the skin causing pseudofolliculitis barbae.” it can also affect trans men on hormones ![]()
https://www.aocd.org/page/PseudofolliculitisB
“Vitiligo is believed to be an autoimmune disease that results in the destruction of melanocytes leading to depigmentation. The disease affects approximately one percent of the population worldwide. Studies have demonstrated that the disfiguring nature of vitiligo causes high psychosocial morbidity.1–3 This is especially pronounced in populations with darker skin tone..”
Conclusion: The excimer laser is a viable treatment for vitiligo and may yield results more expeditiously than other commonly utilized therapies.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3140900/
a black trans woman reflects on the evolution of techniques and lasers.+ nice little back story about electrolysis 3000, which at the time of this writing was electrolysis2000, assuming aquiring a third.
“E2000’s large cash upfront business model unfortunately locks out most transpeeps of color. It’s ironic because the E2000 technique was purported to be effective at clearing African-American facial hair and stopping pseudofolliculitis barbae, aka razor bumps.”
https://transgriot.blogspot.com/2008/12/transsistahs-secret-facial-hair-removal.html
RIP Monica Roberts ^ lets fix this one aspect of society for her!
https://www.npr.org/2020/10/09/922375866/transgender-rights-advocate-and-journalist-monica-roberts-dies-at-58
remember racism is systemic
https://www.businessinsider.com/us-systemic-racism-in-charts-graphs-data-2020-6
Myron Heimlech, Texas Electrolysis Supply, is really who you need to talk to about multineedles- they gather up all the electrology machines online and have probably the most complete collection of machines in the world to choose from. while probably a good person himself, the business model inherently ensures the same way as electrology2000, and states like Ohio, that those most in need will never access treatments. As the industry prioritized its richer white clientelle it moved away from galvanic into thermolysis. MNG machines becoming a rarity increases their value and puts it out of reach. I believe it is doubly dependent on interest from those practicing who would buy the machines for targeted clientele, and therefor extended to the industry by those producing machines, that combined fail the darker toned population. Galvanic is the best thing for black peeps really due to risk of hypopigmentation. So ive started acquiring multineedles too in effort to help people for free under medicaid- medicaid means everyone. this is why im erased, because im dangerous to peoples standard business practices. I’ve sourced 3 other places to find these machines but also at a cost.
“I’m trying to educate you, your right about galvanic being great for black people and that some technicians do have trouble with the curviture, but you are wrong about galvanic being the only current used, we utilize all three. if their skintone is light or the hair vellous we use thermolysis. If their skin is dark and or the hair deep we use blend; and you can lead your current off DC or AC to specialize blend treatments“-Jo Melching
Bono’s own awesome vintage epilator collection :3
i might need to apologize to em one day an have em sign my page in his book, lol.
“The client put her fingers in the tiny cup that contained salt water. The operator would start with, say, 0.2 milliamperes … insert ONE needle. When the second needle was inserted, she would turn up the current to 0.4 milliamperes, and so on. This would “spread” the current and supposedly all needles would conduct the same 0.2 mA. However, if you inserted into a larger/more moist (conductive) follicle, you would get more current flow into that follicle … so it could be very “exciting.” (Modern “computer controlled” units control current to each individual needle.)
[note they removed the “first blend” which was a metallic blimp shaped machine by Kree]
https://hairtell.com/forum/t/electrology-history/40307
“Whether the unit has “auto sense” (i.e., the machine goes “on” when the needle is inserted) … or, if they use a foot switch to turn on the current, there is no difference. It’s like this:
Suppose the therapist sets the DC at 0.5mA. She starts the machine (either by foot, or by auto-sense) the current goes “on” and the amount you get is the pre-selected 0.5mA. And, that’s it.
“Current” usually refers to actual electrons moving through a conductor (in this case your body). “Voltage” is like the pressure needed to push those electrons through the body, (there is always resistance to current flow … unless, I think, you get to absolute zero?). The setting on the meter is a selection of current (or electrons, if you will), that travel in the body.
“Constant Current” means that if you select, say, 0.5mA … the voltage (pressure) will automatically go up or down to maintain that “constant current” flow of electrons.
The important thing? NO WORRIES, if it’s auto or foot switch … same thing.
I think the auto-start works by having an infinitesimal amount of current at the needle all the time. When the machine senses a change in conductivity/resistance (as from “no connection” to “wet body tissue”), the unit switches the current “on.” It’s a nice feature. Again, I might not have this entirely correct.
(Amazingly, there was an unending discussion about whether current goes from + to -, or from – to + Old literature said that there was a “buildup of electrons” at the “plus” pole and then went to the “negative” or electron-deficient pole. Today, it’s just the opposite. And, don’t even read this last paragraph, it’s BS for sure. True, but BS nevertheless.)”- Mike Bono
https://hairtell.com/forum/t/is-the-rod-held-during-electro-supposed-to-be-wet/38910/7
Bono Electrolysis, Santa Barbara, California, still working [no longer teaching]
http://bonoelectrolysis.com/contact.htm


names of multineedle machines to look for
http://temporary3.hammerdata.com/electrolysis-hair-removal-equipment.html
![20201202_151258[1]](https://kittysbelle.files.wordpress.com/2015/10/20201202_1512581.jpg?w=494&resize=494%2C278#038;h=278 "20201202_151258[1]")


Kree^– early 1900s (1906-1915 various dates assigned its invention), model#338. dont believe in afterlife but itd be neat if ghosts were giving me their storys. obviously been collecting multineedles. month or so ago found an old wooden MNG without an arm. today i go lookn, this complete arm and litterature pops up as a new listing, offered, accepted, paid all within like 2 mins. shipped within an hr. like scary handed to me.
“My friend and his father purchased the cabinet and the items you received at a sale.. That stuff was in the cabinet for probably thirty years. They just used the cabinet for storage. I don’t know the lady, I wouldn’t have sent the ladies paperwork but I figured it gave you more history. I thought it quite interesting. Hope you enjoy it. We still have the cabinet.”- Deb




Hoffman^– was eventually bought by kree according to texas, but i believe this happened backward (ive seen that name in a basement befor like they went on to bigger better things) and im going to try to prove it via the evolution of machinery.
RA Fisher Corp., Epilator Model CP-16 – 1980; Ronald Alamo Fisher- “Fishers prinicple”, there are two versions, one with wood sides and one with black plastic sides-the latter matches my CB7.
RAFisher no longer produces electrology devices, they have manuals for the latest, not the older, 800-525-3467
http://510k.medevnet.com/product_codes/index.cfm?fuseaction=companies&product_code=KCW
RCX-Western inc, Epilator, Multiple needle-model EM-20 – 1981
Galvanic medical Instruments, Guibor microelectrolysis unit 18, and Galtel 18- 1980s
https://fda.report/Company/Galvanic-Medical-Instruments-Inc
Alexander Thomas Inc., Microprocessor Contr.Multi-needle, Galvan epilator – 1986![20201202_141014[1]](https://kittysbelle.files.wordpress.com/2015/10/20201202_1410141.jpg)
Gentronics^– jim jensen ,released the gentronic in 1987 and closed in 2012. think theres maybe more than these 3 models: “MC-160 is the analog [pictured], MC-160 D is the digital version, MC-160 S looks like the digital but doesnt have port for mutineedle.”
https://www.hairfacts.com/makers/electro/gentronics-multi-channel-inc/
^thanks to Steve Cooper, heres how to build the lead ribbon off the back of the gentronics up to your individual probe wires..
Gentronics, how to build nerves for the arm



Clare
pre clareblend? 6 finger, clare in a cross
Clareblend, Nova 2000, (the only blend multineedle) 800-334-7126
“Any Clareblend multi needle is no longer made, nor supported. We are currently working on a new model at this time.” OMG! based on inquerys, their making a new galvanic MNG!
http://clareblend.com/nova.htm
^invented by Margarett Smith from reno nevada
https://www.freepatentsonline.com/5797904.html
old single needle galvanic
John Bell & Croyden & Arnold & Sons
https://www.worthpoint.com/worthopedia/early-electrolysis-device-john-bell-94686317

![20210530_204459[1]](https://kittysbelle.files.wordpress.com/2015/10/20210530_2044591.jpg?w=111&resize=111%2C198#038;h=198 "20210530_204459[1]")
![20210530_204629[1]](https://kittysbelle.files.wordpress.com/2015/10/20210530_2046291.jpg?w=110&resize=110%2C198#038;h=198 "20210530_204629[1]")
")
Mahler Superfine model W.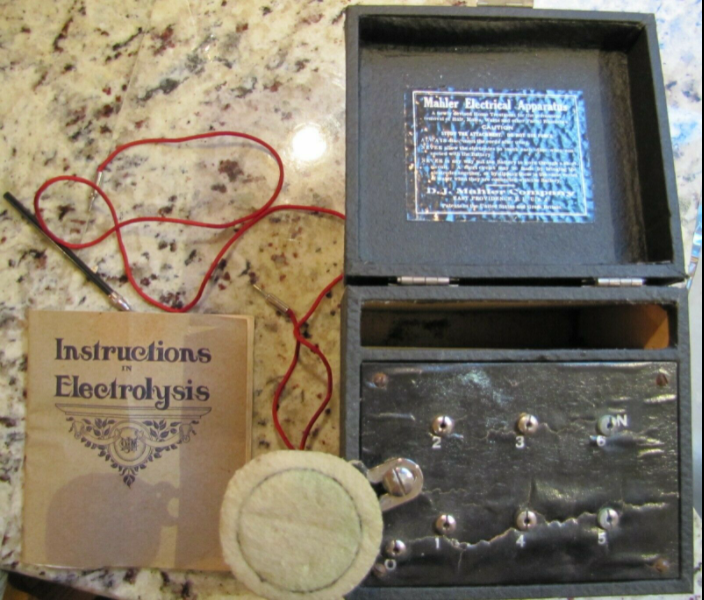
concerning the cute small boxes:“whats that box? why thats the first multineedle, comes with one, but if you had 9 probe cords for each slot and a charged battery..“- Donna Noble
“A while back I ran across a family where the father had passed away, and was a collector of vintage radios, and various other electric gadgets. From them I acquired quite a large number of items, with the understanding that I take it all to get what I really wanted. He lived in the Minneapolis, MN area, and I would guess he bought it at a sale or auction locally. The family didn’t know much about his collection, and I think were surprised at the volume of stuff.
I am interested in restoring vintage (vacuum tube era) radios, amplifiers and test equipment, and so those were the items of particular interest to me.”– thunderthorton
–https://www.worthpoint.com/worthopedia/antique-quack-medical-mahler-electrical-treatment



Electromedica Co Ltd, Bournemouth, Model De Luxe, electrolysis Pencil, 1950s- this device is NOT the “electric pencile” (which looks cool af but didnt work), this an actual galvanic electrolysis device similare to the Mahlers home devices running off a battery with both +and- inputs. MAKE SURE any device old or new has a cathode for return, otherwise its not a complete circuit, therefor its not performing galvanic electrolysis.
“wall plate”-…
“Medicine Battery/Medical Battery“ if you want to go further into machines that will.
“The medical battery was used to provide electrical treatments in the home and clinic for nearly five decades (1870-1920)…Inside the wooden box, a battery was connected to a wire that was wrapped around an iron core, and a second wire—not connected to the battery or the first wire—was also wrapped around the iron core. When the battery was turned on, a direct current was produced in the first wire, thereby magnetizing the iron core. A variety of methods were used to pulse the direct current—causing rapid changes in the magnetic flux of the iron core, thereby inducing an alternating current in the second wire.49 Most medical batteries—which it should be emphasized, refer not just to the physical battery itself but the entire apparatus—provided the primary, direct current (which was referred to as “galvanic” current and came in pulses), the secondary, alternating current (often referred to as “faradic” current), or a combination of both. Even though most batteries provided both direct and alternating current, they were sometimes referred to as “faradic batteries.
“By 1905, mentions of the medical battery in medical journals and textbooks had largely been replaced by references to newer electrotherapeutic technologies, such as sinusoidal-wave producing devices (which produced a smoother type of alternating current via an electric motor)109 and high frequency devices. Although some electromedical instrument manufacturers continued to carry older galvanic and faradic models of their medical batteries, by the 1910s, as on-the-grid electricity made its way into the home, using a battery—instead of plugging into the wall—seemed like an outdated approach, and the medical battery began to slowly fade from medical catalogues.
“That the product has become synonymous with quackery in the world of collectors is an ironic final coda, because as I have shown throughout this paper, the medical battery was the one consumer electrotherapy product not considered as such by medical professionals who practiced electrotherapy. Indeed, the medical battery occupied a unique position, flourishing for nearly five decades both in the domain of medical practitioners and that of home consumers, blurring the boundaries between medicine and consumerism.”
https://academic.oup.com/jhmas/article/72/2/166/3073509
Magnetic induction is the core principle of ^
https://www.prc68.com/I/Faradic.shtml#:~:text=One%20of%20the%20applications%20of,the%20advertising%20that%20was%20allowed.
Multineedle Galvanic Electrolysis (MNG)
“As all manufacturers have CEASED production of multiple needle machines with the exception of one very small manufacturer; students are obviously extremely limited as to what modern multiple needle machines are available on the market and as such; we do not typically train on the multiple needle technique of galvanic any longer since they generally will not be using that older technology in actual practice. We do utilize the more modern single needle galvanic techniques.”
https://www.electrologyschool.org/FAQ_Electrolysis_Training.htm
“However, one persistent difficulty with multi-needle has been the tendency of the needle to slip out of the follicle during the prolonged treatment. The two-piece needles would not stay properly inserted. So Mary went against the conventional wisdom and experimented by using one-piece needles, bending the shaft at about a 30 degree angle. This solves the problem: the needles stay in the follicle very reliably! so the students have begun to do this with all the clients at the Institute’s clinic.
Bending is simple: before placing the probe in the needle holder, take a lip roll, and holding it vertically, insert the blade of the needle into it end-wise. Then bend the needle to the angle of insertion of the follicle to be treated. The angle can always be adjusted later on in the same way – by using a dental lip roll.
Mary recommends avoiding metal-to-metal contact = never use tweezers to adjust a needle. And always take care not to allow the probe chuck to rest on the skin.”
https://synopticproducts.com/2018/12/04/multi-needle-electrolysis-mary-evangelista/
“Few schools specialize in MNG electrolysis, so it’s more of an art form shared between practictioners whom enjoy this modality.”
http://www.emancipatedelectrolysis.com/2015/04/27/modality-wars-thermolysis-vs-galvanic-vs-blend/
“Multi-needle galvanic electrolysis is a highly effective means of permanently removing unwanted hair, however it is time-consuming, requiring at least 3 minutes per hair…Galvanic electrolysis was further developed in 1916, an additional 5 needles were added to the unit to reduce the time required for treatment. This is known as the multi-needle method…The chemical continues its work for a period of time following removal of the needle.”
https://hairfreelife.com/different-types-electrolysis-best/
Multi-Needle providers as of 2020
Electrology3000, Lewisville Texas
https://electrology3000.com/
a patients memoir walkthru of an appointment with Alana Dzurek, a Licensed Electrologist in Beverly Hills.
“I literally fell asleep at one point during the process. I was able to watch myself in the mirror too see watch how the hair came out and I cried laughing because I looked like Frankenstein with the needle wires stuck to my face.”
https://www.bombette.com/health/multi-needle-electrolysis-for-permanent-hair-removal/
Robin Harris, S California
I am a former Electrolysis instructor at the American Institute of Education in Southern California. Dedicated in training new students in art of permanent hair removal. If you are in need of in-home services, please call my secretary for an appointment and explain the nature of your physical care.
https://www.electrolysisbyrobin.com/
Partners in Plastic Surgery, Grand Rapids, Michigan “Multiple needle galvanic electrolysis is FDA-approved for hair removal and can treat all types of hair, skin and areas of the body. It is perfect as a follow-up to laser treatments for those stubborn or white hairs.”- note that VPL is just an improved form of IPL
https://www.pipsmd.com/skin-care/hair-removal/
Amber Rowan, This method is best suited to course, thick hair e.g. beards and all types of body hair.
https://hairfreelife.com/different-types-electrolysis-best/
Susan Rowanburg, Somerset NJ, As a dialysis nurse she observed that patients were growing unwanted hair due to the side effects of the various medications they were receiving.
https://www.electrolysisbysusanrosenberg.com/services
Tracie Disher, Muncie Indiana, 765-747-0668 I instigated, then chaired, the committee for the Indiana Professional Licensing Agency for Cosmetology Examiners (State Board) that wrote the current electrology school rules and regulations.
http://www.electrolysisinfo.com/about-electrolysis-hair-removal.html
Cameo College of Essential Beauty, Utah
https://cameocollege.com/programs/electrolysis/
Cindy Cassady, School of electrolysis health and beauty, Pensecola florida
https://www.electrolysisschools.com/files/133771641.pdf
syndney australia, Permenance hair removal clinic,
“Today’s machines regulate the current distributed to each probe gradually increasing current at the beginning of each insertion and tapering it off at the end. Early machines had no such ability and operators tried all sorts of innovations to ease the jarring sensation of current start-up. A common method was to connect each of the batteries supplying the current in stages and to have the client slowly remove their hand from the saline solution used to complete the circuit before the current was switched off.“
https://permanence.com.au/about-electrolysis/electrolysis/history/
Anita sizemore, panama city florida, does multineedle, “we invest in quality equipment, including the Hinkel and Gentronics epilators, to ensure that your treatment is comfortable, safe, and effective.”
https://electrolysisfl.com/contact-us.html
Susan B. Wash, Brandywine Electrolysis Inc, Wilmington Delaware, medical and cosmetic dermatology she partnered with a laser tech, this is the 3rd mention of using MNG to follow up laser , in such a scenario talk of “length of time for the galvanic current to work” is inconsequential, when comparing a laser/electro regime vs say thermolysis only start to finish. if it truly is less painfull this makes it totes more practical for the clients experience as well.
https://fannyjberg-md.com/Electrolysis
Rejuva, India
http://www.electrolysis.net.in/home/index.php/reyuva-electrolysis/multi-needle-electrolysis-multi-galvanolysis
Patricia Rojas, Patricias electrology Studio, Edmonton Canada, “Only Electrologist in town using a multineedle galvanic epilator Guaranteed permanent hair removal even in stubborn hard to treat areas.”
https://www.linkedin.com/in/patricia-rojas-51a76ab4/?originalSubdomain=ca
Senza Pelo, Oracle of Experience, Arizona, “is part of a new surge in the medical aesthetics industry that specializes in non-invasive procedures. From 1997 to 2013, the number of non-surgical cosmetic procedures performed in the United States increased more than 500 percent,“
https://www.linkedin.com/in/maria-denicola-6b484196/
Jean Raymond, Sydney Australia
“Where there is enough hair to be treated, whether in a single area or over a number of locations, Jean will frequently use two machines. This means 32 probes are used instead of 16.”
https://jeanraymond.com.au/faqs/
Orla Cresswell+ Ysobel Peters, Skin Agents, Gildford Australia, similare to the laser+MNG treatment idea, this organization uses IPL as they also make and sell the IPL devices to the western half. they use all three forms of electrolysis reserving the MNG for the stubbornest of hairs. its actually a nice operation setup they got, sans the IPL focus but it started as a manufacturer and aquired a clinic, they do alot outside of hair removal.
https://skinagents.com.au/electrolysis/
Suzanne Anderer: Illinois School of Electrology
https://www.phrsimple.com/
Simcha Erlich C.E., UK
http://electrolysisbysimcha.com/index.php
Pnina Radbill, LE, NY, MNG/laser
https://pninaluxehairremoval.com/about-us/
Catherine Hayes, Galway, Ireland “Galvanic Electrolysis is the superior choice for body hair and some strong facial hair while the duration of each treatment is longer, regrowth is significantly reduced until it finally ceases to grow. Generally Galvanic takes a quarter to a third of the time regular electrolysis takes to give permanent results.”
http://www.catherinehayesclinic.com/aboutElectrolysis.htm
Soheila Biria, Gentle touch, Rockwood Maryland,
https://agentletouchmd.com/transformations/
Martas Electrolysis, Bethesda Maryland, “You shouldn’t feel the probe’s insertion into your hair follicle, nor should you feel like hair is being pulled out when it’s removed. When properly treated, your hair will slide out of the follicle without any pain.” – note, classifying trans care as a subsect under males is transphobic
https://www.martaselectrolysis.com/male-hair-removal
Essential Electrology, Bloomfield Colorado,
http://essentialelectrology.com/electrolysis/
Janet Sharlach, Chicago Illinois
https://www.linkedin.com/in/janet-sharlach-41949b20/
Sara Picone, Picone Beauty and Wellness Spa, Kennett Square, Pennsylvania
“A soft and effective method for truly removing hair permanently, the galv ep system precisely targets the entire length of the hair follicle and changes the PH of the cells, leaving the hair follicle useless forever. Equally permanent and safe for all skin types and for all hair types and colors…
high-frequency (h-f) method became popular in the USA in the 1930’s and 1940’s …
The galvanic current discharges from the full length of the inserted needle thus destroying the entire length of the follicle. The longer the current is permitted to flow the further the alkaline reaction infiltrates laterally.
The low intensity is sufficient to destroy the targeted tissue with only a mild inflammation reaction in the surrounding tissue. In most adult patients the redness dissipates within thirty minutes. The long, fine, highly flexible needles permit precise positioning and helps insure total destruction of the targeted tissue with only one treatment, insuring no regrowth.”
https://picone1.com/electrolysis
Susan Laird, California, “I left school a firm believer in multi-needle galvanic, but it only took about 2 months to realize that while the 16 channel concept was good, the design left a lot to be desired at the needle end where the tangle of wires and the movement of the patient were a constant annoyance. I found that claims of 900 hairs per hour were difficult to substantiate.
From 1994 until 2000, I favored high galvanic low thermolysis, single needle style of blend electrolysis. It worked well. Since 2000, I have undertaken to improve various aspects of galvanic operation. Galvanic continued to prove far superior to any other method and in 2000, I dropped thermolysis from my practice. Please read my section on Galvanic Electrolysis for more information.”
The continuing effect of galvanic lye in the follicle tissue following the removal of the needle. This continued destruction damages the outer follicle wall as well as any DNA bearing material left in the follicle after the removal of the hair itself.
Continued degradation of Sodium Hydroxide (Galvanic Lye) which is chemically unstable, results in the formation of Hydrogen Peroxide which sterilizes the former follicle site and inhibits the regrowth process of new hair.
The real secret to the power of galvanic electrolysis is the continuing devastation of the hair follicle and regrowth cells after the needle has been withdrawn. When this characteristic is properly exploited, speed can be greatly accelerated, and it is for this reason that my ability to permanently kill a hair follicle is much greater than with any other method.”
thermolysis and laser do considerable damage by disabling the ability of the skin to eject debris by forming scar tissue around the now dead follicle. Encapsulated debris can remain for a lifetime.
http://hairzapper.com/about-me/

this pic is the first and the last galvanic machines ever made + kitty
as the field prioritized its richer-white-clientele it moved away from galvanic, even though it is still the most permanent form of electrolysis and later models were supposedly “painless” compared to the low first pass reduction and pain of thermolysis. multineedle is the rarest form of electrolysis treatment, next and most specialized is blend though a precursory look in your state will find someone within a hundred miles. thermolysis is a dime a dozen, while it takes more insertion skill, its easier on the technician and feels like you got further than your really did with its high regrowth. If i could find anouther technician, using 2 multineedle machines we would be as fast as blend, with the highest kill rate.
![IMG_20201015_213952[1]](https://kittysbelle.files.wordpress.com/2015/10/img_20201015_2139521.jpg)
new freindy :3, Audrey Jones, from Washington sent me her old probe wires for the Gentronics, Thank You!
https://www.pnwelectrology.com/
oh! shes made some videos of her working with it! ❤
https://www.youtube.com/watch?v=SghLK0IHnKA
![20210402_001418[1]](https://kittysbelle.files.wordpress.com/2015/10/20210402_0014181.jpg) bought an older thermolysis machine from ebay but weary of using it myself without training, spose i got to start somewhere, but i know ill scar myself learning insertions. “My dad and my uncle liked everything Brown. That one you’re holding was a little flamethrower.”-Skip Mahler
bought an older thermolysis machine from ebay but weary of using it myself without training, spose i got to start somewhere, but i know ill scar myself learning insertions. “My dad and my uncle liked everything Brown. That one you’re holding was a little flamethrower.”-Skip Mahler
“those run hot”-Carol Hawkins, talking about older Instantrons.
DIY kids should be starting on galvanic, not thermolysis* (Ive since updated options to a Blendtone; while i quest for multi-needles- the RAFisher cb7 is the mate to a multineedle, and found an artifact card- Gentronics. Been reading, having collected most every textbook on the topic yet there so much yet unread. have had talks with a handful of licensed electrologists in and from diffrent states, so feel as if i have a good understanding of theory and concepts of an ethical practice.


![20201202_141014[1]](https://kittysbelle.files.wordpress.com/2015/10/20201202_1410141.jpg?w=298&resize=298%2C167#038;h=167 "20201202_141014[1]")
a study done using my first machine the ss-69 epilator from Instantron; the article uses disgusting terminology being from 1997 (the 90s weren’t kind, and youll still find oldworld transphobic viewpoints expressed in these books, some even used currently as school curricula) in general the author stresses the need for a good electrologist, whose successfully treated trans women before and how done wrong can be no reduction.
http://dallasdenny.com/Writing/2013/05/12/electrolysis-in-transsexual-women-a-retrospective-look-at-frequency-of-treatment-in-four-cases-1997/

experience with using a mirror’s reflection-by mantaray
“This has always been a big thing in my mind that I have wanted to undertake. I remember reading posts by Aliciadarling. She was a pro, but also did DIY and commented on her experiences. She was doing face, and had mentioned that the toughest challenge was getting the angle off the skin (theta angle? z-axis?) correct. She said that getting the insertion wasn’t the hard part, it was coming in at the correct angle.
Area:chest, Setup: I got one of those automobile dashboard accessory bendable things that allow you to attach one end with a suction-cup to the windshield, and the other end hold your cell phone. They have about 8 inches of sturdy bendable flex cord. I put a 7-inch diameter mirror on the suction end of that, and the other end attached to the boom mic stand.
Tips: Keep the mirror perfectly horizontal to minimize interfering angles.
Use the long handpiece
Keep solely focused on the mirror, and nothing else.
Be prepared to use a variety of holding styles and switch from left to right.
Also keep your light source directly above. Blocking my own light was an issue.
you’ll get more prominent eschars most likely because the inserts aren’t as clean. Be delicate with the insertions and very mindful before hitting the footswitch, watch the dimpling levels, finding the botton of the follicle is not a problem. it was easier to get the insertion than to extract the hair with forceps afterwards. I found the insertions happening quickly when I just stared at the follicle and let the hand do it’s own guiding. And after I returned to normal working style on a different bodypart, I found myself blazing with auto-insert, because ‘normal’ seemed so much easier.
Hope this helps someone sometime like Aliciadarling’s posts helped me.” -83/148, 2012
https://hairtell.com/forum/t/diyers-areas-goals-concerns-and-progress/38767/83
WARNING everyone ive spoken too has told me DO NOT attempt to do your own face.

Whose original name was Mahler, they sold home galvanic devices from the late 1800s up until restrictions on the feild started. under pressure from a competators school who used a lawsuit and the FDA in 1974 to claim DIY hair removal was “too dangerous” even though itd been perfomed for a hundred yrs in hirsute womens mirrors.
Skip Mahler- “The small bottle on the lower left of the picture is called Ninex. I am guessing that this was a topical anesthetic used for treatments. The name of that product was named after my grandmother, whose nickname was Ninon. Her name was actually tio Linda Machado from Portugal. She came for treatment to the United States from my grandfather, they fell in love and got married, and had many children. When her first child was born, Daniel II, when he started speaking he could not pronounce the name Mother. He would continually say Ninon, So the name stayed with her for the rest of her life. Myself and all her other grandchildren called her this name only.” is an ethical source for needles regardless what machine your using, because they really did bring electrology to the layperson, making it about as democratic as its ever been.
http://instantron.com/product-category/electrolysis-machines/instantron-epilator-accessories/needles/
you need to keep your electrolysis equipment calibrated, this is Instatron’s new site and skip can work on a few different models.
http://instantron.com/?page_id=50
june 30 1953, kree was officially ordered by the FDA to desist claims of 100%accuracy using a “kree radiomatic” shortwave device, use of “research bureau” that implies kree had such staff, claiming its the only device when its not, or that it is “guaranteed for life” – 8391
https://www.ftc.gov/sites/default/files/documents/commission_decision_volumes/volume-49/ftcd-vol49july-june1953pages1587-1650.pdf
1956 kree misused a winners bio of an essay contest, to make it look like she operated their equipment when she did not, judgment for the plantiff.
https://www.leagle.com/decision/1956238233f2d51236
Kree Institute of Electrolysis, Inc. filed as a Foreign for Profit Corporation in the State of Florida and is no longer active. This corporate entity was filed approximately fifty years ago on Wednesday, June 30, 1971 , according to public records filed with Florida Department of State. It is important to note that this is a foreign filing. A foreign filing is when an existing corporate entity files in a state other than the one they originally filed in. This does not necessarily mean that they are from outside the United States.
https://www.corporationwiki.com/New-York/New-York/kree-institute-of-electrolysis-inc-3381221.aspx
“There not only is some evidence to support this finding, but there is factually sufficient and substantial evidence to show that the employer Kree’s dissatisfaction was not genuine but was feigned. From the record it may reasonably be inferred that Mrs. Fageros was terminated not because of any performance that was unsatisfactory or detrimental to the business, but to make a place for the more experienced electrologist from the other Waco shop.”- lawsuit by Betty Fegerous in 1972
https://www.courtlistener.com/opinion/1632014/kree-institute-of-electrolysis-inc-v-fageros/
1977, kree filled for a gavanic powered timed thermolysis machine with an antenna as the cathode, that did normal probes and the infamous electric tweezer scam, “A dual epilator for removal of unwanted hair. Line power is reduced and rectified in a power supply which energizes a timer circuit and an RF amplifier. A timed DC pulse emitted from the timer circuit under an operator’s regulation feeds a normally unenergized crystal controlled oscillator whose output is boosted in the RF amplifier. The RF power can be selectively utilized by a needle or tweezers. A tuned antenna provides an efficient return for the RF power.”
https://www.freepatentsonline.com/4167187.html
ohnos! he started getting those fake lawsuites when he lost a couple real ones  this lady claims that she was harmed by not only his machine they used but the technician he trained. thats what killed em all the legal fees 😦
this lady claims that she was harmed by not only his machine they used but the technician he trained. thats what killed em all the legal fees 😦
https://casetext.com/case/cremeens-v-kree-inst-of-electrolysis though Paul Kree, of the Kree Institute of NY, was a viscous selfish business man, with at least 4 lawsuits against em, his ingenious work experimenting with ways to manipulate a complete circuit (passed though the body) helped develop the familiar handheld cathode used today. this “Radiomatic”, may be the harbinger of blend merely having 2 currents separate. to date it: thermolysis was invented in 1923..“there was no timed to thermolysis device until 1948..”-Skip. the time control on this machine is for the galvanic, meaning its between 1923-1948. remember Paul Kree did not invent blend, but did develop the galvanic multineedle- which used liquid metal cups as the anode: where a patient could dip one finger in one cup at a time time to slowly increase even controle the current, at the same time the operator would hook up batterys in series for a slow build up, when treatment was over they would do the series in reverse. this model is corded, missing its patient ground,( thought it was the side bar i mistook) thats actually the base for the missing MNG arm. -“wish i could. I got it from the trash, believe it or not. I pick for a junk company and kept it. I love this piece, it’s just so cool. The little red and green plastic plug in spots are definately bakelite. I think you’ll love it. I want to say that i saw paper work from Red Bank NJ for an office when i was doing that job. Hope that helps.”|
though Paul Kree, of the Kree Institute of NY, was a viscous selfish business man, with at least 4 lawsuits against em, his ingenious work experimenting with ways to manipulate a complete circuit (passed though the body) helped develop the familiar handheld cathode used today. this “Radiomatic”, may be the harbinger of blend merely having 2 currents separate. to date it: thermolysis was invented in 1923..“there was no timed to thermolysis device until 1948..”-Skip. the time control on this machine is for the galvanic, meaning its between 1923-1948. remember Paul Kree did not invent blend, but did develop the galvanic multineedle- which used liquid metal cups as the anode: where a patient could dip one finger in one cup at a time time to slowly increase even controle the current, at the same time the operator would hook up batterys in series for a slow build up, when treatment was over they would do the series in reverse. this model is corded, missing its patient ground,( thought it was the side bar i mistook) thats actually the base for the missing MNG arm. -“wish i could. I got it from the trash, believe it or not. I pick for a junk company and kept it. I love this piece, it’s just so cool. The little red and green plastic plug in spots are definately bakelite. I think you’ll love it. I want to say that i saw paper work from Red Bank NJ for an office when i was doing that job. Hope that helps.”|
this is what the wooden kree would look like resurfaced, beautiful!
https://www.pinterest.com/pin/650559108652758351/
other state schools verifying Ohio’s Legislative/DoH corruption
“Ohio has a 750 hour electrology training requirement and at the present time, American Institute of Education does not support or offer this curriculum. Ohio is one of only a few states that requires out of state vocational schools to become “state approved” with Ohio’s State Medical Board and the Directors of AIE decided that there wasn’t sufficient reason to pursue this requirement. We also disagree with their curriculum to some extent. The curriculum requires 150 hours of head and neck massage training, something that no other state requires and that no electrologist would consider doing. If you plan to practice electrology in Ohio upon completing your training, we suggest that you attend a school in this state.
If you live on the border of a neighboring state and plan to work there rather than in Ohio, or, if you are planning to move from Ohio to another part of our country, call our Director, Ron Davis at 888-844-4247. AIE trains students for most other states in our nation and we would be pleased to assist you.”
https://www.aielectrology.com/Ohio.shtml
^they do have a scholarship towards going to their school. should apply even if it wont help me in ohio. they do have something they call a “walking degree” that is basic education for the 16 or so states that dont require licensure.
http://www.aielectrology.com/scholarships.shtml
^ so that school in California replied saying i should just do school in Ohio without giving much to go on but to look here in the http://electrology.com/contact.html (which im emailing a rep in Ohio from the contact us page) inquired again with the Cali person an they got me a link to a new school opening in columbus on a hairtell forum —–contacted the area educational chair and they gave me links to the one in cbusMary Kaye Johnson mkjelectrolysis@aol.com
 “Your message was forwarded to me regarding the electrology training programs in Ohio. The American Electrology Association is not a regulatory body so the information provided is simply a list of the known schools in Ohio. You should call both schools with your list of questions and go from there. That said, please feel free to call me with any general questions regarding training. The AEA website at www.electrology.com has information regarding the CPE designation. If you click on the Professionals page, there is a link on the left hand side of that page with info on becoming a CPE along with the CPE test bulletin. Wherever you train, you should plan to take the exam and become a member of the AEA in order to stay on top of continuing education opportunities and be involved with the wonderful peer networking opportunities.”
“Your message was forwarded to me regarding the electrology training programs in Ohio. The American Electrology Association is not a regulatory body so the information provided is simply a list of the known schools in Ohio. You should call both schools with your list of questions and go from there. That said, please feel free to call me with any general questions regarding training. The AEA website at www.electrology.com has information regarding the CPE designation. If you click on the Professionals page, there is a link on the left hand side of that page with info on becoming a CPE along with the CPE test bulletin. Wherever you train, you should plan to take the exam and become a member of the AEA in order to stay on top of continuing education opportunities and be involved with the wonderful peer networking opportunities.”
“From what I recall I found it in the bottom of a jewelry box in Sun City, AZ a large retirement community. I dont really know anything about the previous owner as they seldom share info about them. I dont recall anything of consequence to be honest. Sorry couldnt be of more help. The fact the name was changed at some point I found interesting but never was able to confirm exactly when that may have happened.”-Dano
so far one of the only electro schools in America that takes federal school loans is in salt lake city utah
sent timid interest thingy waiting to hear back 🙂 no hear back 😦 and heard its course structure is set up to use you as free labor (lota practice) without teaching theory.
sent another email and didn’t mention anything about Ohio, got a reply…
“Good Morning Jayla.
This is Cyndle with Cameo College Admissions. Thank You for your inquiry. The Electrolysis industry is a fantastic industry to get into 🙂 I can definitely help you w/ your FAFSA, have you ever filled out one before?
I would suggest coming into Cameo College. When you come I will give you a tour of the campus, go over course curriculum, and tuition. I will also help you fill out your FAFSA at that time 🙂 I am available Tues – Sat is there a day of the week that works best for you?
“You can never be overdressed or overeducated.” ― Oscar Wilde
Cyndle Mendoza
Cameo College Admissions Advisor
801-747-5705 Direct Line
801-747-5701 Fax
the hatefull Mormon social culture of Utah 😦 mentioned because that’s where cameo college is- BUT they DO teach you on MNG!
http://www.advocate.com/current-issue/2016/4/29/ghost-children-mormon-country
Whoot! Found a school that takes fed loans in massachusettes! Electrology Institute of New England , and guess what? Omg they refuse to let me in!? this is there reply, caps an all
” Hi JAYLA EINE IS AN ACCREDITED SCHOOL WE HAVE HOMELAND SECURITY APPROVAL FOR INTERNATIONAL STUDENTS, IT WAS EASIER TO OBTAIN THAN APPROVAL FROM OHIO FOR OUR ELECTROLYSIS PROGRAM. WE HAVE MADE MANY REQUESTS TO THE STATE OF OHIO HOWEVER WE HAVE HAD NO RESPONSE. UNTIL WE DO WE DO NOT WANT TO TAKE MONEY FROM ANYONE OR FROM THE DEPARTMENT OF EDUCATION UNTIL WRITTEN APPROVAL IS RECEIVED. WE HAVE APPROVAL FROM ALL OTHER STATES, WE DO OFFER FINANCIAL AID THROUGH THE DEPARTMENT OF EDUCATION. PERHAPS YOU CAN HAVE YOUR ELECTED OFFICIALS LOOK INTO THIS TO SPEED THINGS UP. OUR INITIAL REQUEST WAS SOMETIME AGO. PERHAPS AS A RESIDENT YOU WILL HAVE MORE OF AN ADVANTAGE TO GET THINGS ACCOMPLISHED. ” BEST WISHES, MARY EVANGLEISTA, DIRECTOR
so im left to educate myself..
![20191108_115005[1].jpg](https://kittysbelle.files.wordpress.com/2015/10/20191108_1150051.jpg?w=4032)
“Another important thing to consider is whether the electrologist treats you like a patient or a bag of money. I felt that the electrologists that would put a timer, check the time every second or try to make me sign a contract that said to come at least two times a week as a client or she wouldn’t be able to treat me were being unfair and were thinking of getting paid more than treating me. I honestly did not like that as I knew that I would be doing treatments for a long time and wanted an electrologist that I could trust and that wasn’t just in it for the money. The one I go to now schedules me for a session of however long and sometimes pass the time scheduled by 2-10 minutes and she never charges me. I think she knows that there is a lot of work to do and she treats me more like a human being, rather than a bag of money. She always makes sure that whatever area we’re doing that day is completely hair free.”
https://www.mypcoskitchen.com/pcos-facial-hair-electrolysis/
Bureau of Vocational Rehabilitation
every state has one, (im told by the go between for the ohio electrolysis association and the DoH, whose currently charging 140 an hr and the only “electrologist” left-everyone else are “cosmetic therapists”), that theres an offchance the BVR might at least partially pay my way thru school, like they did her mom. they gota cause it only hope 😦 but i dont have connections like those who created these barriers- classic battle of trans girl vs the machine, an its eats us for lunch everyday.,. ,. .,. .. , .
https://ood.ohio.gov/wps/portal/gov/ood/individuals-with-disabilities/services/vocational-rehabilitation
anyhoo so i meet with a “caseworker” for Warren county Ohio’s BVR, she seemed ok at first but sorta defeatist. we were spose to develop a business plan and present it to columbus in hopes of approval. she says we need statistical evidence of jobs and industry placement for what im trying to do….3 months later and she still hadnt got back with me so i filled grievance and she could meet next day; where she used a half hr befor hand to dismiss the need for a trans competent electrologist using a “job scale”
even when told its self employed. so i filed grievance higher, who sent me higher to the director of Warren BVR who immediately found the schools the worker had said she couldn’t find, and gave me a list of things ill need to accomplish if i can access the BVR thru a “better county.”
2020 i finally got far enough away from cincinnatis bigotry in social services that i might be able to actually access some of them! so wish me luck as i approach the BVR representative we now have on campus 🙂
5/17/21- refered to North Central, Connie Ion who just spoke with them now claims “not to do vocation services” after realizing im the trans kid their killing.
6/17/21- refered to Southeast health, which is also ADAMH funded and after 2 weeks of no reply via email
These three academic health networks need an electrologist; University of Cincinnati Dermatology, Ohio State University’s devision of plastics and reconstructive surgery, and Cleveland Clinic’s LGBT center. been cutting a swath across the state in search of healthcare.
heres where we are after 5 yrs, (odds are your state doesnt have these barriers, this is ohio specific), how there is no electrologist in state willing to work with medicaid, explained in 2 screenshots.. its the 93 OAC amendment to the 92 ORC code, that gives it a zero reimbursement rate under medicare services in state. she simply cant be guaranteed of reimbursement, shed be signing up blind- which id do for another but is completely understandable. this law is now illegal according to contractual obligations to receive federal funding. We have medicaid oversight following this case, its eventuality that they realize the same.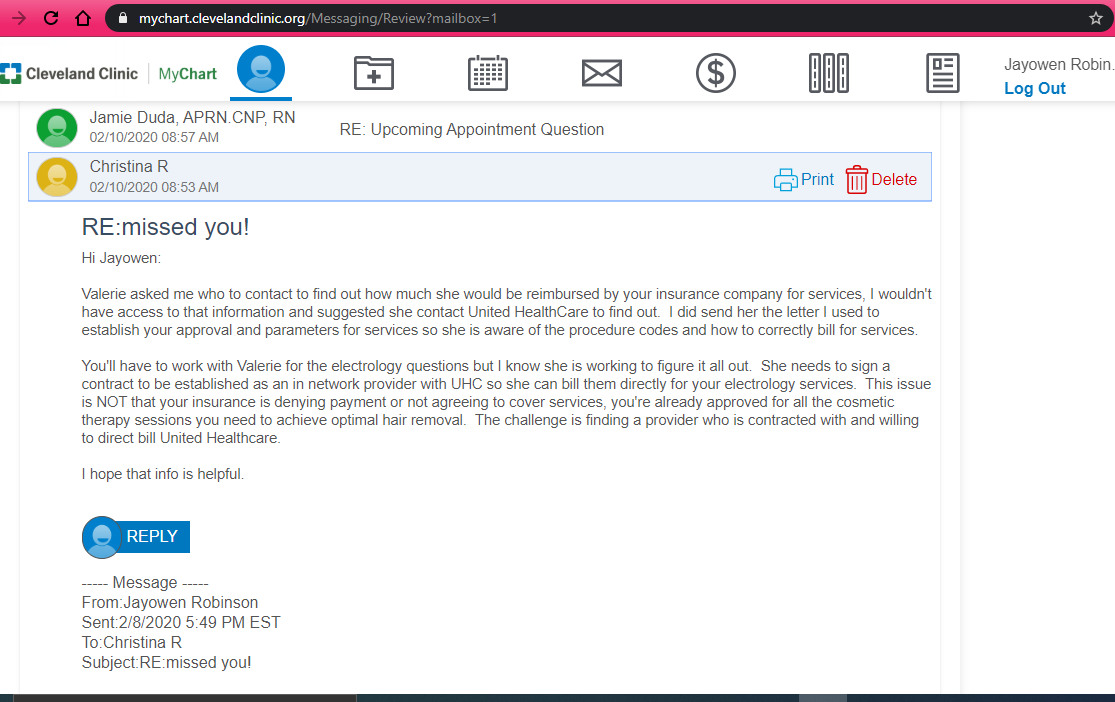
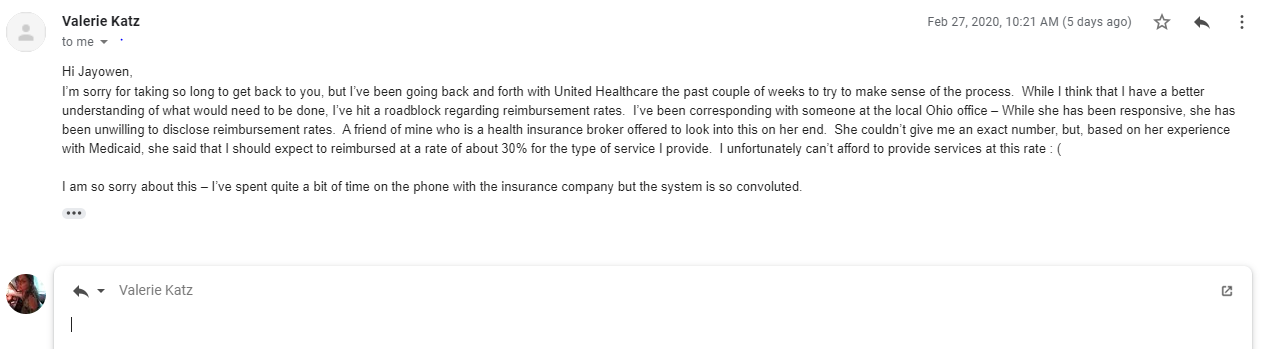
Guidance for the management of hirsutism. NCBI,- “Approximately 80% of women are affected by the presence of excessive hair growth. Excessive facial hair in particular can be a source of distress to such women and can lead to psychological problems such as anxiety, depression and a reduced quality of life.Current cosmetic methods of hair removal include shaving, depilatories, waxing, plucking, laser, intense pulsed light (IPL) and electrolysis. A topical treatment cream such as eflornithine 11.5% can slow hair growth and thus reduce the frequency of the need for hair removal. This treatment can be used effectively in conjunction with hair removal methods.
http://www.ncbi.nlm.nih.gov/pubmed/16083532
Sex Change Surgery Market Will Surge at 25% CAGR to hit USD 968 Mn by 2024
“In the last few years, public awareness regarding transgender and gender nonconforming (TGNC) population has reached unprecedented heights. Increase in awareness and resources regarding transgender issues and accessibility related to gender reassignment surgical procedures have resulted in boosting the demand for sex reassignment surgeries. The transgender healthcare concern is rising and experiencing considerable surge in interest from several healthcare providers and policy makers. “
https://www.prweb.com/releases/sex_change_surgery_market_will_surge_at_25_cagr_to_hit_usd_968_mn_by_2024/prweb15996165.html
so also found this ISBS seems to be some business savy statistical thingy 🙂 i wonder where i find access to getting the full readout?
Hair & Nail Salons in the US: Market Research Report
IBISWorld identifies 250 Key Success Factors for a business.The most important for the Hair & Nail Salons Industry are
Business expertise of operators [was almost a non-profit once +ethics]
Having a loyal customer base [pre-op is an intimate adventure as well you get to know your technician over the hrs spent together in pain,lol]
Access to niche markets [a trans competent electrologist in Ohio working with medicaid would dominate]
https://www.ibisworld.com/industry/default.aspx?indid=1718
Hair Loss Treatment & Removal in the US: Market Research Report
“Over the five years to 2016, industry revenue is expected to grow due in part to the rising emphasis consumers have placed on physical appearance. Aging males seeking hair loss treatment and females seeking hair removal services dominate industry demand. Over the five years to 2021, revenue for the Hair Loss Treatment and Removal industry is projected to grow at a slightly more subdued rate
https://www.ibisworld.com/industry/default.aspx?indid=1720
Plastic Surgeons: Market Research Report
“Interest in cosmetic surgery continues to climb as technological advancements make procedures more accessible, more affordable and safer. Cosmetic surgery is no longer reserved for the wealthy or famous; most cities in the United States are home to plastic surgery centers, offering body contouring procedures, such as liposuction and breast augmentation; facial rejuvenation, such as eyelid surgery and chin and cheek implants; laser hair removal; and other enhancement procedures.
IBISWorld identifies 250 Key Success Factors for a business. The most important for the Plastic Surgeons Industry are”
- Educating the wider community [most of the market is geared towards cisgender]
- Adopting new technology [afflicted, understanding hair issues, pain management and the value of various techniques]
- Easy access for clients [creates a direct route to access care that currently doesnt exist]
https://www.ibisworld.com/industry/plastic-surgeons.html
here’s a nice one with multiple different stat sources for the field of plastic surgery
http://valuationresources.com/Reports/SIC8011PlasticSurgeons.htm
Surgeons report nearly 20 percent increase in number of transgender surgeries
https://www.lgbtqnation.com/2017/05/surgeons-report-nearly-20-percent-increase-number-transgender-surgeries/
^ a talk with Dr Ting from Mount Siania in NY who’s pioneering advancements in GRS, talks to the need and lack of surgeons available, started first fellowship, for first time in 2017 theres a place for surgeons to train. the field is more open, more sharing of techniques n procedures.
http://www.slate.com/articles/podcasts/working/2017/12/how_does_gender_reassignment_surgeon_jess_ting_work.html
anouther thing for the BVR is interviewing 2 practicing electrologists
electrolysis works! blog by an elder technician
https://electrologyworksnow.com/2014/02/10/becoming_an_electrologist/
Amy Day from Oakwood Electrolysis, in Dayton, is THE BEST electrologist ive ever had work by. She understands pain like no other, having been afflicted herself at one point, meaning she kinda started learning the same way i am- from the other side of the probe. instead of considering pain an inevitability when trying to push thru when the patients uncomfortable to get clearing done, she knows exactly when to letup, resulting in the most therapeutic and comfortable sessions ive ever experienced (even if i still cried couple xs,lol). She humored me on 7/19/17..thank you Amy ❤ for your time!
https://www.oakwoodelectrolysis.net/
1) How long did schooling take?
“1yr, 705 hrs.”
2) How much did school cost?
“$6,000”
3) Which school did you attend?
“Columbus Medical Electrology Institute, since closed 15 or so yrs ago.”
4) Did you recieve any finacial assistance?
“As it is proporietary, no. private finaces, a second morgage.”
5) How many clients do you serve?
“Starts out on an individual bases and builds as you go, dont expect to pay yourself for the first 2 yrs.“
6) Would you describe electrology as a fulltime or partime vocation?
“Its like working 2 jobs sometimes, fulltime.”
7) Are you part of any networked association?
“Cosmetic Therapist Associacion of Ohio (CTAO)”
8) Do you know of any apprenticeships?
“In Ohio, no. you have to go to a school and take a state exam to become liscenced by the Medical Board.”
9) How long does it take to earn back the cost of schooling?
“Theres alot of factors that go into a business, for instance: your overhead on rent will between 200-1000 dollars my own is a 3 yr contract, all your products from antiseptic to sterilization, all your paper-sheets-etc need replaced and or laundered after each client, to the unknown as you venture into marketing.”
10) How long does it take to build fulltime clientelle?
“That will be up to the individual depending on who you target as clientele.”
11) How far do you commute to work?
“30 mins”
12) after liscencing by the state, what other legal restrictions would one face concernign location for operations?
“Outside the state each county sets up their own operating restrictions.”
13) What of liscencing out of state?
“it is not unknown that somone went to KY and failed the OH state exam”
14) In addition to schooling and material, what other costs do electrologists face?
“Utilities and insurance: malpractice is suggested, health and accidental is mandatory.”
15) Is there anyhting else you would suggest in preperation and consideration of entering the feild?
“you get what you put into it, prioritize it.
– Take some small business classes.
– Seek partnership with anouther already established electrologist.
– Keep politics out of the treatment room.
– Always place medical befor the art aspect of electrology.
– Spend some time focusing on your professional look, beyound your wardrobe (she rocks scrubs); is your office cluttered or sterile, what does your business card say about you, what takeaway do your clients have?
– Maintain one singular phone number for the future of the business, even if you move locations, because clients will suggest you to friends yrs after treatment or come back themselves at a later point.
– keep track of all finaces, from any help to expenditure, keep a spreadsheet so you can see and show anouther how much youve spent and gained.
After 15 yrs into this i can tell you that you will always have good months and bad months, scheduling and time management is key.“
The following is a talk with Laura Bomar, shes in tennessee
“Takes about 3 to 5 thousand to get started right in this business.”– Laura Bomar (thanks 🙂
https://www.facebook.com/laura.bomar.3
Johanne Fortier CPE, LE, National Training Director, Laura trained with her in California and she trains students for unlicensed states. She runs a business called Aesthetics Systems and works mostly with Dectro products.
http://www.aestheticssystems.com/
Lighting


“Get a daylight lamp,some cheap ones at joane called Ott lite” http://www.ottlite.com/Our-Story/Dr-Ott-The-Original or verilux which is what laura has http://www.verilux.com/
“Prestige, is an electrolosis supply store sells things like magni specs”
https://www.prestigeelec.com/shop/magni-specs/magni-specs
“Texas Electrolysis Supply, is another supplier of everything, both sell needles an whatever.”
http://texaselectrolysisstore.com/
^texas’s 2009 digitaly archived brochure [look further into!]
https://docplayer.net/42614444-Table-of-contents-june-2009.html
Sterilization
a) Adequate professional indemnity and public liability insurance is considered obligatory.
b)best means of avoiding cross-infection is to use disposable equipment where available, in preference to other types. c) needs to be emphasised that ultrasonic equipment only cleans but does not sterilise instruments.
d) internal parts of the structure of the premises should be maintained…The surface of the floor should be continuous. hand basin with a hot and cold water supply and properly connected to the drainage system is essential and should be located in the electrologist’s work room; water heaters of the “top-up” type are not permitted. It is preferable for the taps to be foot or elbow operated.
c) table tops, shelves and other working surfaces must have a smooth impervious surface (preferably stainless steel or glass}, be in good repair and kept clean with the frequent use, at least once each session, of a suitable disinfectant. Shelves, cabinets, cupboards, etc must contain only equipment that is used in connection with the business of the electrologist.
d) surface of any chair, seat or couch should have a smooth impervious surface such as vinyl etc. in good repair. Patients should sit or lie on a disposable paper [or change seating covers for each client] Fabric chairs should not be used.
e) Ventilation shall be such as to provide a minimum of six air changes per hour
f) A suitable standard over all for the premises would be 500 lux with a higher level of 1,000 lux “free from
glare” at all working areas in the treatment room
https://assets.ctfassets.net/ii3xdrqc6nfw/Xg0cHrxyc68KCMq8o6Gy6/6c7bc97be0c33c27051e868351c9f9f5/Code_of_Practice_Electrolysis.pdf
“An autoclave or dry heat sterilizer is required by the CDC for sterilizing the instruments like tweezers though. pricey item, a dry heat sterilizer by Wayne is 500 or so. You’ll have to have the proper sterilization before working on anyone. That’s for your safety. You will also want to be certain to get Hep shots and other shots/vaccinations required for healthcare workers.”
http://www.waynemetalproductsinc.com/



^ found a vintage Norelco dry heat sterilizer and got a Bransonic ultrasonic cleaner (typically used for fine tuning oils for guns) these make great pretreatment to knock off debris before being put in the sterilizer – you probably don’t need one this big as its a gallon of water to turn it on -figured if ima’ have one might as well be able to do bigger pieces; they do make smaller plastic ones size of your eyeglasses, an even ones for whole feet!
![20201225_000332[1]](https://kittysbelle.files.wordpress.com/2015/10/20201225_0003321.jpg) “you’ll need a pump bottle for the alcohol and many people use witch hazel for after care use.”
“you’ll need a pump bottle for the alcohol and many people use witch hazel for after care use.”
70% rubbing alc is used for prep, as anything stronger evaporates before it can enter a bacterial cell, it itself is a disinfectant, that cleans out and opens up the follicle.
Witch Hazel, used for aftercare is an astringent, that contstricts the follicles, closing them up while protecting them from microbial repopulation.
The best thing for aftercare isn’t Neosporin, but keeping the area clean and dry as it heals.

“There are some probe companies that will send free samples.” laura uses Sterex probes, but “there are different brands and everyone has their favorites,” got some free samples of probes from Pro Tec last year.”
Prestige supply is sending me samples of all their deepest probe options 4/20/21 (also got the Shuster videos from them)-“The Telangiectasia probes are going to be roughly the same length as the regular probes, but are meant for spider vein treatments and are not appropriate for use for hair removal. The probe you are using should be the same width as the hair you are treating. A 2-3 would be good for fine hair, 3-4 for an intermediate hair and a 5-6 for a coarse hair. Some probes like Prestige Premier and Sterex come in a couple different lengths (Short and Regular) to help electrologists treat those deep and shallow hairs effectively.
https://www.prestige-supply.com/about/
![20210415_183341[1]](https://kittysbelle.files.wordpress.com/2015/10/20210415_1833411.jpg) “Laurier probes are the best in quality and they are also the most expensive. They spend a bit more time developing these probes and may have some detailed information that will help. Electrologist who use these probes often charge a bit extra to cover the cost. I use Laurier for the galvanic and Sterex for thermolysis. But, everyone is different. It’s a bit overwhelming”
“Laurier probes are the best in quality and they are also the most expensive. They spend a bit more time developing these probes and may have some detailed information that will help. Electrologist who use these probes often charge a bit extra to cover the cost. I use Laurier for the galvanic and Sterex for thermolysis. But, everyone is different. It’s a bit overwhelming”
http://www.laurierinstruments.com/kelly-tip-electrolysis-probes.html
“When the cable is placed around your neck, the wires that connect the cable to the probeholder are kept straight…to store your probeholder, roll it in a wide circle to avoid compressing the wires.” also includes a how to hold a probe for insertions video.
https://aestheticssystems.com/blog/tips-to-extend-your-probeholder-lifespan/
she has the Oakworks Wellspring Portable Massage Table. “It is made so that legs can fit underneath it. Most massage tables don’t allow for that, so make sure your legs can fit under whatever table you decide on.”
http://www.oakworks.com/wellspring.asp
“I would charge more for bikini area than face, because it’s more difficult and harder on your back to manipulate the area around the bikini. Watch your posture, too! That’s a big issue with electrologists….big issues. Go to any length to keep your posture as good as possible – it will save your back, neck and many types of health side affects. Posture is something I have to work on. I got this great gadget that I positively love… “
https://www.lumobodytech.com/posture-correctors/
Thank you Laura ❤
****
for those undergoing SRS/GRS/GCS this is a drawing from the Michigan Gender Clinic on what areas need to be free of any dirty stitches befor surgery can happen. copy paste if it doesnt show up as a link.
file:///C:/Users/Hp1/Downloads/ElectrolysisDiagramRedrawn.pdf
^ if that link doesnt work it can also be found in the group on FB, DIY hair removal but i was erased befor its censorship was noticed by mainstream society.
https://www.facebook.com/groups/1020380451379215/files/
the backup group due to FB nazi censors is on MEWE but its more of a temporary quiver for things unread
grants and funding for inclusive resources
trans ohio-symposium, i think this is wher you would present your ideas in hopes of finding funding for your LGBTQIA non profit or business? *it did help me evolve, thank you.
http://www.transohio.org/?p=17
trans justice funding project
http://www.transjusticefundingproject.org/
mellinial fund
http://www.ohio.com/news/local/millennium-fund-grant-supports-program-that-helps-transgender-youths-1.643995
apalachian regional commision
http://www.arc.gov/funding/ARCGrantsandContracts.asp
Society for reproductive investigation, you have to join the society an pay dues to be eligable but they are the same ones doing genetic testing on transsexuals so deserve it.
https://www.sri-online.org/career-development/sri-grant-programs
native grant, I have native blood, my greatgreatgrandma but my current grandma says “they liked to dress like Indians” as dig to me an refused to meet me to discuss the genealogy she built, running off pictures that took a months sallary in the day,lol. If I can prove that it opens me up to grants for school and other benefits
http://www.ancestry.com/cs/offers/freetrial?ftlp=1&o_iid=48816&o_lid=48816&o_sch=Web+Property
might have to do a DNA test
https://www.ancestry.com/dna/?s_kwcid=ancestry+dna+com&gclid=Cj0KEQiA5bvEBRCM6vypnc7QgMkBEiQAUZftQCQiY_tN_LVo7-OzOsAn9eWWnsIQTXFmSG8o217pq1QaAuU-8P8HAQ&o_xid=58712&o_lid=58712&o_sch=Paid+Search+Brand
scholarships
nice compilation of scholarships for LGBT people!
http://www.affordablecolleges.com/resources/lgbtq-college-resources/
point foundation lgbt scholarship if your in school
https://pointfoundation.org/point-apply/apply-now/
trans studies scholarships an fellowships
http://davievillagepost.ca/5973/donations-sought-for-uvic-transgender-studies-scholarships-fellowships/
2,000 feminist writers
https://www.freedomwithwriting.com/freedom/uncategorized/2000-feminist-writing-fellowships-from-bitch-media/
disability vocational training might find a grant for electrolysis school ?every state has it
http://www.ood.ohio.gov/Core-Services/BVR
AOTC tax credit for first 4 yrs of school, 2,500 per yr of documented expenses
https://www.google.com/webhp?sourceid=chrome-instant&ion=1&espv=2&ie=UTF-8#q=AOTC
IRS school first 4 yrs 2,500 deductable
https://www.irs.gov/uac/american-opportunity-tax-credit-questions-and-answers
Duane Gordon, Middletown community foundation
Our rules don’t allow me to pass around any requests to people but we might be able to help. Twice a year we take applications for nontraditional students (meaning people age 25 or older going back to school). I’m not sure which of our funds are open for trade-School type classes like this or which ones are restricted to more standard associates and bachelors degrees in college, but you might qualify to be considered for those scholarships. Can’t guarantee you’ll get anything, but if you don’t fill out the application and try, you’ll never know! The application becomes available online June 1 at mcfoundation.awardspring.com. The typical award is between $500 and $2,000 per semester. You have a to reapply each semester. The application is due July 1 for fall semester and December 1 for spring semester. https://mcfoundation.awardspring.com/
if anything was useful, or ya’ care, here’s my fundy meh’ to go to school. it was letting me have my own pre-op work here and there before realizing the level of corruption. now its anything initially used for survival or aquisition of tools to insert myself into the machine. eventually matches a savings acct that floats equal to or towards it at any given time . 10-20k is what i need to buy my way into the corrupt field of electrology in Ohio just to help my people for free 😦 https://www.gofundme.com/kittysbelle
if this ever becomes a paper in a medical article:
1- footnotes after period
2- citation before period
3- section break first then header and footers
fun! AEA extended this research, that’s what i want you all to do apply this in every state. shity of em out trans an intersex issues with it though, afterterall its where she got it when i told their director about ohio overegulation, noticed an responded to on 2/27/21
Ricardo Azziz, M.D., M.P.H., M.B.A., Professor Departments of Obstetrics and Gynecology, and Medicine, The University of Alabama at Birmingham, Birmingham, Alabama and Teresa Petricca, CPE, Executive Director, American Electrology Association.
Continuing Education![20210223_004533[1]](https://kittysbelle.files.wordpress.com/2015/10/20210223_0045331.jpg)
https://silo.pub/principles-and-practice-of-electrical-epilation.html

4 thoughts on “Medical Necessity of Electrolysis/ Laser/ Permanent Hair Removal”